Christopher
Holt June 8, 2018
This week
the Social Security and Medicare Trustees released their annual
reports on the financial health of their respective programs. The reports are a
combined 530 pages, but fear not faithful reader, AAF’s own Jonathan
Keisling and Tara Hayes have broken out the key
findings for you in a much more manageable six-page document, available here. Now I’ll summarize it for you in nine
words: both programs are headed for a meltdown, and fast.
Social
Security will be unable to meet its obligations by 2034, and Medicare Part A
will be similarly situated by 2026. Don’t get too hung up on the specific
year—these numbers move around a bit from report to report based on various
factors. The important point is that American entitlement programs face a
reckoning within the next fifteen years or so. We’ve overcommitted these
programs and the time to address this problem is now, not in the future.
Now, as
Sam Baker wrote for Axios yesterday morning, “Cutting
Medicare benefits is unpopular; so is raising taxes to pay for Medicare.” So,
it’s not like there are easy answers. But if we don’t change the benefit
structure, we will have to make some draconian decisions on revenue. Let’s take
a quick look at what it would have required to balance Medicare’s budget in
2017.
Medicare
Part A ran a cash flow deficit last year of $35 billion. To make the Part A
trust fund balance, we’d have needed to increase the payroll tax that funds it
by 13 percent. Medicare Parts B and D are funded by a mix of premiums and
direct payments from the federal Treasury. By law, premiums can only account
for 25 percent of total Medicare spending. But for purposes of demonstrating
the scale of the problem, let’s imagine we were going to make Parts B and D
whole through premium increases. Medicare Part B ran a cash flow deficit of
$232 billion in 2017. To balance the Part B budget, we would have needed to
increase Part B premiums by 285 percent. The average Medicare beneficiary would
have seen a $4,583 increase in their annual premiums. And what about Part D?
The 2017 cash flow deficit for the drug program was $85 billion. To balance
that disparity, beneficiary premiums would have needed to increase by $2,354,
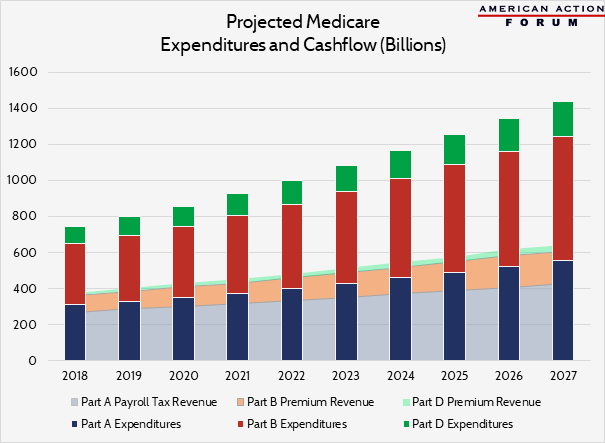
or 545 percent. The chart below shows how these deficits play out over the next
decade, absent program reforms or the kind of taxes and premiums outlined here.
It’s not pretty.
In the
midst of this crisis—and it is a crisis—many on the political left are
proposing expanding Medicare’s liabilities through
extravagant “Medicare for all” proposals. Perhaps we should first focus on
ensuring there is still a Medicare program at all for anyone in future years.
Chart
Review
Jonathan Keisling, Health Care Policy Analyst
Jonathan Keisling, Health Care Policy Analyst
The graph
below illustrates how low Medicare’s projected premium and payroll tax rates
are relative to expenditures and, implicitly, the resulting burden on the trust
fund and treasury. To ensure hospital payments can continue to be made beyond
2026, cash flows must, at the very least, reflect expenditures. Part A payroll
tax revenues would need to increase by an average of 21 percent over the next
10 years.
No comments:
Post a Comment