Christopher Holt September 7, 2018
You’ll be unsurprised to learn that
policymakers, health insurers, and consumers worry a fair amount about health
insurance premiums. As a result, those in health policy circles spend a
significant amount of time thinking about what drives health insurance premiums
and what can be done to reduce them. Sometimes events totally outside of one
policy silo, however, sneak over and gum things up in another. Such is the case
with Dodd-Frank and health insurance premiums.
In the aftermath of the financial crisis, there
were efforts on both sides of the Atlantic to prevent similar troubles from
afflicting the financial sector in the future, with the United States passing
the Dodd-Frank financial reform act. Thomas Wade, AAF’s director of
financial services policy, has written a helpful piece explaining
the process by which the United States and Europe have sought to align
regulatory frameworks but, in so doing, may have done U.S. health insurers a
disservice.
Health insurance as it exists in the United
States doesn’t have a direct corollary in most EU countries. Further, health
insurance functions differently than other forms of insurance, and the industry
is not dependent on investment performance or large capital holdings to pay out
claims. This is where Dodd-Frank comes into play—read Wade’s piece for a more detailed
exposition of the history. For our purposes, though, the primary issue is
something called “group capital requirements,” which the Federal Insurance
Office—established by Dodd-Frank—is implementing as part of an agreement with
European regulators.
A capital requirement is simply the amount of
reserve capital an entity is required to keep to ensure it can meet its
obligations and does not become insolvent. But group capital requirements are
problematic for health insurers. Wade explains that the group capital
requirement being demanded by EU officials, in the case of health insurers,
would “also presumably factor in non-health subsidiaries. Extremely low risk
health-related service entities – for example, those that provide medical IT –
will also be assessed as part of this calculation. Overnight, health insurers
will appear to be undercapitalized for entirely artificial reasons.”
The implications of this should be clear: Costs
for U.S. insurers will rise, and those costs will be passed along in the form
of higher premiums to consumers. This tradeoff might be worthwhile if it made
sense for health insurers to be subject to a group capital requirement, but it
doesn’t. The present situation is being driven by a combination of lack of
understanding of the U.S. health care system across the Atlantic, and an
apparent lack of awareness among U.S. regulators of the implications of the
policy for health insurance.
CHART REVIEW
Jonathan Keisling, Health Care Policy Analyst
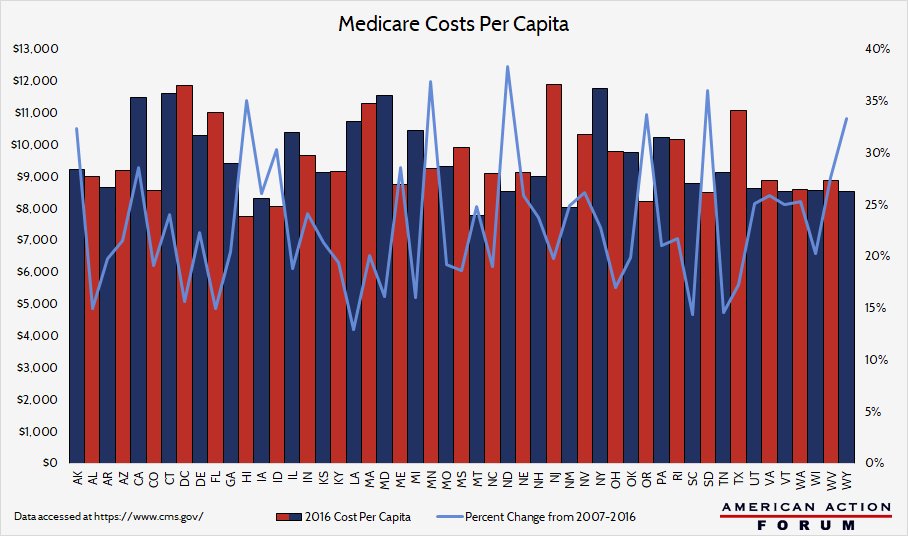
Policymakers have long faced the problem of
geographic variation in health care costs. The graph below provides an overview
of the geographic variation of health care costs by looking at each state’s
Medicare costs per capita. New Jersey has the highest costs per capita and
Hawaii has the lowest. While a useful starting point, this approach could
understate or overstate costs, as the numbers reflect both costs and need—thus,
New Jersey could have expensive care or a needy population, or (more likely) a
mix of both. This graph indicates that several mid-Atlantic and New England
states and California have high relative costs, but the data merit further
inquiry.
FROM TEAM HEALTH
Research: Understanding The Social Determinants Of Health
The United States overall takes a medicalized approach to health care, emphasizing medical treatment over other factors that influence health. Deputy Director of Health Care Policy Tara O’Neill Hayes and Rosie Delk examine the various “social determinants” of health and look at their implications for public policy.
The United States overall takes a medicalized approach to health care, emphasizing medical treatment over other factors that influence health. Deputy Director of Health Care Policy Tara O’Neill Hayes and Rosie Delk examine the various “social determinants” of health and look at their implications for public policy.
WORTH A LOOK
FierceHealthcare: Montana Health Co-op notches a victory
in lawsuit over cost-sharing subsidies
Wall Street Journal: Walgreens to Offer Allergy Treatment
Auvi-Q as EpiPen Shortage Persists
Axios: Tennessee Blues to stop covering OxyContin
Disclaimer
https://www.americanactionforum.org/weekly-checkup/financial-crisis-and-health-insurance-premiums/#ixzz5Qi2pVn4d
Follow: @AAF on Twitter
https://www.americanactionforum.org/weekly-checkup/financial-crisis-and-health-insurance-premiums/#ixzz5Qi2pVn4d
Follow: @AAF on Twitter
No comments:
Post a Comment