Christopher
Holt November 9, 2018
If you’re wondering what the Democratic takeover
of the House and the slightly larger Republican majority in the Senate mean for
health care policymaking in the immediate future, the short answer is: probably not that much.
The current Congress
has reached something of a legislative stalemate when it comes to major health
initiatives, and the elections were not going to change that
reality. True, the 115th Congress has seen some
accomplishments on health care. Some of those—e.g. opioid legislation—did not
depend on unified party control of both chambers. Others—such as the repeal of
the individual mandate penalty and delays of many Affordable Care Act (ACA)
taxes—stretched the Republican majorities almost to their breaking point. But
Congress couldn’t repeal the ACA during the 115th, and Republicans
likely wouldn’t have been able to do so in the forthcoming 116th even
if they held the House. Similarly, Congress couldn’t reach a deal on an individual
market stabilization package, and again there wasn’t much reason to believe the
election would change that. The
margins in the House and Senate, and the divisions within the GOP conferences,
weren’t going to change enough to open up a path to partisan bicameral
policymaking even if the GOP had held the House.
Ultimately, major policymaking in health care over the next two years will take place
within the agencies through the rulemaking process. In fact, much of the
significant policymaking already has been occurring through agency actions.
(See recent examples here, here, here,
and here.)
Again, this would have been the case regardless of party control. So, when it
comes to new health care policies during the 116th Congress,
look to the Department of Health and Human Services.
All this is not to say
that the Democrats’ return to power in the House is irrelevant. The administration will find itself facing
aggressive opposition in its rulemaking efforts, especially when related to the
ACA. Perhaps more important will be the way that a Democratic House shifts the
policy conversation. Medicare-for-All
and other single-payer initiatives will gain valuable,
profile-raising debate time in House committees and even on the House
floor. There may also be an
opening for legislation on prescription drug prices, as the president’s
policy preferences on that matter already lean in the direction of the House
Democratic caucus.
The Democrats will find legislating difficult,
though, just like Republicans did. Most of the actual policymaking over the
next two years will happen in the executive branch.
CHART REVIEW
Tara O’Neill
Hayes, Deputy Director of Health Care Policy
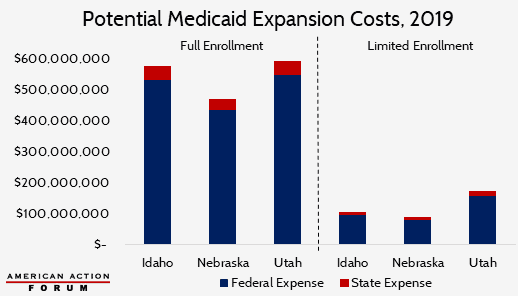
On Tuesday, residents in three states voted to
expand Medicaid eligibility, bringing the total number of expansion states to
37 (including the District of Columbia). In 2019, the federal government will
fund 93 percent of each state’s Medicaid expansion costs, before declining to
90 percent in 2020 and each year thereafter. The following chart shows
estimates of the potential range of costs for each of these states in 2019. On
the left is the cost if all eligible individuals (119,000 in Idaho; 86,000 in
Nebraska; and 158,000 in Utah) take advantage of the new opportunity. On the
right is the cost if only those in the “Medicaid
coverage gap”—i.e. those caught between current Medicaid eligibility
and ACA subsidy eligibility—enroll. The resulting numbers create a likely upper
and lower bound for the annual cost of expanding Medicaid in these states.
https://www.americanactionforum.org/weekly-checkup/what-does-the-election-mean-for-health-care-policy/#ixzz5WsQ4JKZE
Follow @AAF on Twitter
No comments:
Post a Comment