Tara O'Neill Hayes November 28, 2017
Executive Summary
Twenty-five years after Congress created the
340B Drug Pricing Program, policymakers are actively considering important
reforms. While the program is rooted in good intentions, it suffers from a lack
of much-needed oversight, resulting in several problems. Rapid expansion of the
program in recent years is adversely affecting patient access to
community-based, affordable health care, in direct contradiction to the
program’s mission. Patients are too often not benefitting from the mandatory
discounts provided under the program. The amount of charitable care provided by
hospitals has declined considerably in recent years, despite being one of the
primary reasons for establishing the program. Reforms are needed to ensure
program integrity and sustainability.
Introduction
The 340B Program was created to help ensure that
uninsured and low-income individuals have access to prescription drugs.
Congress created this new program after another federal program—the Medicaid
Drug Rebate Program—caused drug manufacturers to pare back dramatically their
charitable donations of such medicines.[1] Since
its creation, the 340B Program has expanded considerably. Part of this
expansion is due to an outdated eligibility threshold for hospitals, which
makes hospitals more likely to qualify for 340B as they treat fewer uninsured
patients and more insured patients. As more providers become eligible for the
program’s mandatory discounts and the availability of those discounts spreads
beyond the low-income and uninsured individuals the program was designed to
help, the health care market grows more distorted, adversely affecting more
than just prescription drug prices.
The House Energy and Commerce Committee recently
held a hearing examining the current status and
impact of the 340B Program. During that hearing, lawmakers expressed concerns
with the program’s rapid growth and lack of oversight as well as the resulting
negative consequences throughout the health care market.
Background
If a drug manufacturer wants to have its drugs
covered by Medicaid, it is required to participate in both the Medicaid Drug
Rebate Program and the 340B Drug Discount Program. The Medicaid Drug Rebate
Program requires drug manufacturers to provide rebates for drugs prescribed to
Medicaid beneficiaries such that Medicaid is entitled to a drug’s “best price” among most private and
public payors (with certain government program exceptions).[2] The 340B Program requires drug manufacturers
to provide discounts for all of their covered outpatient drugs purchased by an
eligible health care facility for any “qualified patient.” The mandatory
discount for each drug is in the form of a ceiling price, set by a statutory
formula tied to the value of the Medicaid rebate. The discount can be so large
that it results in a price of zero or even a negative price; in these cases,
manufacturers have been instructed to use the “penny pricing policy” and set
the price at one cent.
There are no rules regarding how the savings
obtained through this discount must be used, although there are two explicit
prohibitions for participating entities. The first is known as “diversion”:
340B-purchased drugs may not be diverted to ineligible patients.[3] The
340B Program defines a “qualified patient” so broadly, though, that almost any
patient treated at a qualifying “covered entity” is eligible.[4] The
second prohibition is on obtaining “duplicate discounts” for a 340B drug. This
would occur if the covered entity purchases a drug at the discounted 340B
price, provides such drug to a Medicaid patient, and then submits a drug claim
(or allows the claim to be submitted on its behalf) to the state Medicaid
agency to bill the manufacturer under the Medicaid Drug Rebate Program.[5] However,
because there are no requirements that the discount be passed on to the patient
or her insurer, 340B providers may retain the full amount of the discount,
which averages at least 22.5 percent of the average sales
price.[6]
Growth in the Program
The types of entities eligible to participate in
the 340B Program has expanded several times since the program’s inception, most
recently through the Affordable Care Act (ACA). The ACA expanded 340B even
while allowing an estimated 20 million individuals to gain health insurance
coverage, which should have decreased the need for this program.[7] Eligible
facilities now include multiple types of federally-funded health centers and
specialized clinics, as well as children’s hospitals, critical access
hospitals, disproportionate share hospitals (DSH), rural
referral centers, sole community hospitals, and free-standing cancer hospitals.[8]
After the first 13 years of the 340B Program,
only 583 hospital organizations participated.[9] The
repeated eligibility expansion resulted in the number of participating
hospitals growing to more than 2,000 by 2014, accounting for more than 45
percent of all acute care hospitals.[10] The
continued growth, along with the thousands of federally funded health centers
and clinics that also participate in the Program, brings the total number of
unique covered entities to more than 12,000, as of 2016.[11] This
growth is largely because of the financial incentives for participating
entities and the inappropriate metric used—the DSH percentage—to determine an
entity’s eligibility, as explained here.[12]
Hospitals’ adoption of “child sites” has further
fueled this expansion. Each participating hospital may own multiple facilities,
each of which qualifies as a participating entity, even though on its own the
facility may not qualify. When accounting for the child sites of all the
participating hospital organizations as well as the other qualifying entities,
there were more than 42,000 340B sites as of November 2017, including nearly
19,000 DSH sites.[13]
This map shows the number of 340B entities in
each state, as of November 2017.
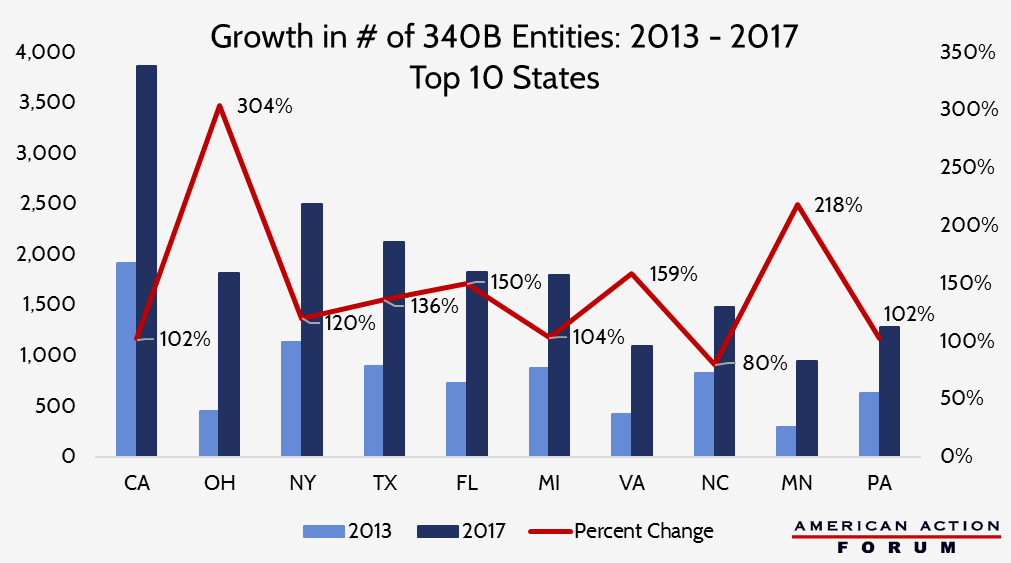
The chart below shows the ten states which have
seen the greatest increase in the number of 340B entities over the past four
years.
Changes to regulatory guidance in March 2010
permitted entities to expand the reach of the program even further through the
use of contract pharmacies. This allows entities to contract with multiple
outside pharmacies to dispense 340B drugs to eligible patients.[14] The
growth has been tremendous: in just three years, the percentage of covered
entities using contract pharmacies under 340B more than doubled from 10 percent
to 22 percent; the number of unique pharmacies with which they contracted grew
770 percent; and the total number of such contracts grew 1,245 percent.[15] Analysis
published by the Drug Channels Institute found that the number of contract
pharmacy locations had grown to nearly 20,000 by 2017. Four large, for-profit
national chains make up 60 percent of these pharmacies: Walgreens (32 percent),
CVS (10 percent), Walmart (9 percent), and Rite Aid (8 percent).[16]
Not surprisingly, as more and more entities have
become eligible for 340B, the share of drugs purchased at a discount has grown
as well. The overall share of outpatient brand-name drugs purchased under 340B
has reached nearly 8 percent this year, up from 5.4 percent in 2012.[17] Sales
under the program have grown at average annual rate of 31 percent since 2013,
and reached an estimated $16.2 billion in 2016.[18]
Impact: Perverse Incentives and Unintended
Consequences Drive Up Treatment Costs
Hospital Profits From 340B
It has become clear that many entities are
taking advantage of the program’s lax rules and lack of oversight. When the
Office of the Inspector General (OIG) for the Department of Health and Human
Services (HHS) investigated 340B DSH hospitals, only one-third reported that
they offer the 340B discounted price to uninsured patients.[19] The
OIG also found that because Medicare has been reimbursing 340B hospitals at the
typical rates without factoring in 340B discounts, in 2013 Medicare Part B and
beneficiaries paid 58 percent more than the ceiling price for 340B drugs. For
35 drugs, the beneficiary’s 20 percent coinsurance alone was greater than the
acquisition cost of the drug. The difference between the acquisition cost and
the Part B reimbursement rate for five high-cost cancer drugs examined by the
OIG among non-340B entities was always less than $1,000, while the spread for
the same drugs at 340B entities ranged from nearly $6,000 to more than $13,000.[20] One
study found that hospitals could make a roughly 500 percent profit off of a
340B drug relative to what the manufacturer who invented and produced it would
earn.[21] In
total, the difference between the hospitals’ acquisition cost and the
reimbursement amount allowed hospitals to retain approximately $1.3 billion in
2013 from 340B discounts alone.[22] The rule issued by the Centers for Medicare
and Medicaid Services (CMS) in November 2017 is an attempt to change this
disparity and ensure that taxpayers and Medicare beneficiaries actually do
benefit from this mandatory discount.
Because of the large discounts, providers also
lose the incentive to prescribe lower cost medicines. This leads to higher
costs for the insurer (or taxpayer in the case of Medicare or Medicaid) and
higher cost-sharing for patients. Studies have found that 340B hospitals
prescribe more high-cost drugs and more drugs overall. One study found that,
among the top five therapeutic categories, the rate at which 340B entities or
their contract pharmacies dispense generic drugs is significantly lower for
340B prescriptions than all other prescriptions in the same therapeutic class.[23] A
report from the Government Accountability Office (GAO) found that per
beneficiary expenditures for drugs covered under Medicare Part B were higher
for patients at 340B DSH hospitals than non-340B hospitals,
even after accounting for the patients’ health status.[24]
While the intent of the 340B Program was to
provide participating entities with a greater ability to provide more charity
care, hospitals are under no obligation to use the funds derived from the
program for charity care. Only 24 percent of 340B hospitals, which represent 45
percent of all hospital beds, provide 80 percent of all charity care delivered
by 340B hospitals.[25] Nearly
40 percent of 340B DSH hospitals provide charity care equal to less than one
percent of their total patient costs.[26] Only
42 percent of tax-exempt, non-profit hospitals informed patients, according to
one study, “of their eligibility for charity care before attempting to collect
medical bills and only 29 percent had begun charging uninsured and
under-insured patients rates equivalent to private insurance and Medicare
rather than standard, higher chargemaster rates.”[27] A
follow-up study found that “only 37 percent of 340B hospitals limited their
charges for patients who were eligible for charity care to amounts generally
billed to insured patients,” and “less than 62 percent… regularly notified
patients of their potential eligibility for charity care before initiating debt
collection.”[28]
Conversely, a recent change in statute created a
discrepancy that disadvantages certain (mostly rural) hospitals and the
patients they serve. Section 2302 of the ACA excludes drugs designated by the
Food and Drug Administration (FDA) for treatment of a rare disease or condition
from being available for purchase at the discounted 340B price solely by
children’s hospitals, free-standing cancer hospitals, critical access
hospitals, rural referral centers, or sole community hospitals; other 340B
entities do not face such an exclusion.[29] It
is important to note that such a designation may be provided to a drug that has
already been approved for a common condition if the manufacturer is seeking
approval for a new indication for a rare disease. There are 450 such drugs
which have been approved by the FDA, but there are currently more than 4,300
drugs that have been “designated” and are thus unavailable for the discount at
these particular hospitals.[30]
Provider Consolidation and Increased Costs
Beyond Prescription Drugs
The 340B discount incentivizes hospitals to
acquire physician practices and make them “child sites” in order to increase
the number of drugs that can be purchased under 340B, as the evidence above
shows. This consolidation reduces the number of community practices and
consequently drives up the cost of care for all services at those facilities,
relative to the cost of the same services provided in non-hospital-owned
physician offices. Studies have shown that consolidation among hospitals and
other health care facilities leads to higher costs at hospitals, often by as
much as 20 percent and sometimes by as much as 40 percent.[31]
The loss of independent community oncologists is
driving up the overall cost of cancer care, contributing to our
unsustainable national health care expenditures. The
actuarial firm Milliman found that the percentage of chemotherapy infusions
delivered to Medicare beneficiaries in hospital outpatient departments (HOPDs)
increased from 15.8 percent in 2004 to 45.9 percent in 2014, with the
proportion of these infusions occurring in 340B HOPDs increasing from 3 percent
to 23.1 percent.[32] This
led to estimated increased expenditures of more than $4,000 per Medicare
beneficiary.[33]
The impact on cost is not exclusive to the
Medicare population, either. The Milliman study found that infusions delivered
to commercially insured individuals in HOPDs rose from 5.8 percent to 45.9
percent during the same period. This site of care change translated to
increased costs of up to 40 percent per day.[34] A
study by the Moran Group found that when treated in HOPDs, a patient was on
chemotherapy treatment 9 to 12 percent more days, compared with those treated
in a physician office. Thus, for patients receiving 12 full months of
chemotherapy, Avalere found treatments in HOPDS cost 53 percent more than the
same treatment in a physician office.[35] Besides
the increased cost, patients spend more days in treatment, rather than at home,
negatively affecting their quality of life.
Negative Impact on the Non-Target Population
The discounts mandated by the 340B Program and
other government regulations may also be responsible for the steady climb in
the list price of prescription drugs. Just as private insurers pay more to
compensate for Medicare and Medicaid’s low payments, the 340B program has grown
so large for certain drugs that their prices are likely climbing as a result of
340B discounts, forcing the rest of the population to subsidize the cost of
these discounts.[36]
Reforms Needed
The Health Resources and Service Administration
(HRSA) and drug manufacturers have been permitted since the program’s inception
to audit 340B entities’ records if there is suspicion of either diversion or
duplicate discounts. Though, manufacturers face severe limitations and must
bear the costs of such audits.[37]
At the recommendation of the GAO after it found
the possibility of widespread non-compliance, HRSA began conducting risk-based
audits of covered entities in 2012.[38] In
fiscal year 2016, 76 percent of 340B DSH hospitals that were audited were found
to have at least one adverse finding and 41 percent had multiple adverse
findings.[39]
Increased use of contract pharmacies has led to
further integrity problems in the 340B Program. The OIG found that contract
pharmacies complicate entities’ efforts to prevent both duplicate discounts as
well as diversion of 340B drugs to ineligible patients. The OIG found that most
entities do not conduct all of the recommended oversight activities, and
one-fifth of those studied do not have any method in place to prevent duplicate
discounts from occurring.[40]
While not every entity is abusing the program
and taking advantage of its patients, the preponderance of evidence shows a
clear need for significant reform and stronger oversight to ensure program
integrity. Currently, only federally funded health centers and clinics are
typically required to disclose publicly how they use the savings received from
the 340B Program discounts. Hospitals should face similar obligations.
Alternatively, 340B hospitals should be required to pass the savings directly
to the qualifying patients. Hospitals claim the savings they receive are put to
good use, and this is true to a degree.[41] Taxpayers,
however, deserve to know that the tax benefit received by these not-for-profit
hospitals is justified. Once these rules are updated, penalties for
non-compliance must also be enhanced. The current response—temporary
ineligibility—does little to deter bad actors.[42]
Another reform should focus on eligibility for the
program. The metric for determining an entity’s eligibility for the program
should be adjusted to ensure participating hospitals are primarily serving the
targeted beneficiaries. The current definition is based on the share of
low-income, Medicare and Medicaid inpatients at a hospital,
but the program provides a discount for drugs provided to outpatients and
is intended to be used for uninsured individuals which, of
course, does not include Medicare and Medicaid beneficiaries. More, the
calculation does not include the percentages of patients at hospitals’ child
sites, which further skews the eligibility metric. This mismatch results in
many entities inappropriately benefitting while other entities with much
greater amounts of charity care do not. Along these same lines, a clearer and
stricter definition of an eligible patient is sorely needed. The current
definition is too broad and allows for many more drugs to be obtained at a
discount than originally intended.
Finally, HRSA needs both more authority to
promulgate regulations that will bring the program in line with its roots as a
safety net program and additional resources to provide sufficient oversight.
HRSA does not have the authority to require hospitals to report the amount of
funds they generate from the Program or how those funds are spent. HRSA also
does not have the authority to share ceiling prices with state Medicaid
programs, so that the states may ensure they are not paying duplicate
discounts.[43] Use
of a 340B claim identifier could likely help in this regard. Additionally,
despite there being more than 12,000 covered entities and 7,000 contract
pharmacy arrangements, HRSA has only 22 full-time employees dedicated to
overseeing the 340B Program, primarily due to a lack of funds and direct hiring
authority.[44]
Conclusion
It is no secret that the 340B Program no longer
seems to be serving its intended purpose and warrants substantial reform. While the program was created to
resolve an unintended consequence of the Medicaid Drug Rebate Program, it has
created its own unintended consequences. The program suffers from a lack of
appropriate standards for program eligibility, clear guidance and requirements
regarding the use of savings generated, and necessary program oversight to
ensure participants are held accountable and the targeted patients actually
receive a benefit. Congress should reform the 340B Program to restore its
original intent, ensure program integrity, and eliminate the harmful market
distortions caused by it. Without such reforms, the program is unsustainable
and the rest of the health care market will continue to suffer.
[6] http://www.medpac.gov/docs/default-source/reports/may-2015-report-to-the-congress-overview-of-the-340b-drug-pricing-program.pdf?sfvrsn=0
[9] http://www.medpac.gov/docs/default-source/reports/may-2015-report-to-the-congress-overview-of-the-340b-drug-pricing-program.pdf?sfvrsn=0
[10] http://www.medpac.gov/docs/default-source/reports/may-2015-report-to-the-congress-overview-of-the-340b-drug-pricing-program.pdf?sfvrsn=0
[11] https://www.federalregister.gov/documents/2017/05/19/2017-10149/340b-drug-pricing-program-ceiling-price-and-manufacturer-civil-monetary-penalties-regulation
[17] https://www.thinkbrg.com/media/publication/928_Vandervelde_Measuring340Bsize-July-2017_WEB_FINAL.pdf
[28] https://www.thinkbrg.com/media/publication/789_Vandervelde_Hospital_Charity_Care_Compliance_Trends.pdf
[36] R. Conti and M. Rosenthal, “Pharmaceutical
Policy Reform — Balancing Affordability with Incentives for Innovation,” N
Engl J Med 2016; 374:703-706.
[38] https://www.hrsa.gov/sites/default/files/opa/programrequirements/policyreleases/auditclarification030512.pdf
https://www.americanactionforum.org/research/340bmarketdistortions/#ixzz5ZZoNWW46
Follow @AAF on Twitter
No comments:
Post a Comment