Meredith Freed , Jeannie Fuglesten Biniek Follow @jeanniebin on
Twitter , Anthony Damico , and Tricia Neuman Follow @tricia_neuman on
Twitter Published: Jun 21, 2021
Medicare beneficiaries have the option of
receiving their Part A and Part B Medicare benefits through a private Medicare
Advantage plan. Since 2011, the federal government has required Medicare
Advantage plans to cap out-of-pocket spending, and these plans may provide
additional benefits or reduced cost sharing compared to traditional Medicare.
They are also permitted to limit provider networks, may require prior
authorization for certain services, and sometimes carry an additional premium
on top of the monthly Part B premium all Medicare beneficiaries pay. This brief
provides current information about Medicare Advantage premiums, cost sharing,
out-of-pocket limits, and supplemental benefits, as well as trends over time.
Two companion analyses examine trends in Medicare Advantage enrollment and Medicare Advantage plans’ star ratings and federal spending under the
quality bonus program.
Nearly two-thirds of Medicare Advantage
enrollees pay no supplemental premium (other than the Part B premium) in 2021
In 2021, 89% of individual Medicare Advantage plans offer prescription drug
coverage (MA-PDs), and most Medicare Advantage enrollees (90%) are
in plans that include this prescription drug coverage. Nearly two-thirds of
beneficiaries in individual Medicare Advantage plans with prescription drug
coverage (65%) pay no premium for their plan, other than the Medicare Part B
premium ($148.50 in 2021). However, 15% of beneficiaries in individual MA-PDs
(2.6 million enrollees) pay at least $50 per month, including 5% who pay $100
or more per month, in addition to the monthly Part B premium. The MA-PD premium
includes both the cost of Medicare-covered Part A and Part B benefits and Part
D prescription drug coverage. Among the one-third of all enrollees in an
individual MA-PD who pay a premium for their plan (6.0 million enrollees), the
average premium is $60 per month. Altogether, including those who do not pay a
premium, the average individual MA-PD enrollee pays $21 per month in 2021.
Premiums paid by Medicare Advantage enrollees
have declined slowly since 2015
Average Medicare Advantage Prescription Drug
(MA-PD) premiums declined by $4 per month between 2020 and 2021, much of which
was due to the relatively sharp decline in premiums for local PPOs, which fell
by $7 per month. Since 2016, enrollment in local PPOs has increased rapidly as
a share of all Medicare Advantage enrollment, corresponding to broader availability of these plans. Average premiums for HMOs
declined $2 per month, while premiums for regional PPOs increased $1 per month
between 2020 and 2021.
Average MA-PD premiums vary by plan type,
ranging from $18 per month for HMOs to $25 per month for local PPOs and $48 per
month for regional PPOs. For all MA-PDs, the monthly premium is $21 per month
for both Part A and Part B benefits and Part D prescription drug coverage (and
averages $12 for just the Part D portion of covered benefits). Nearly
two-thirds (60%) of Medicare Advantage enrollees are in HMOs, 35% are in local
PPOs, and 4% are in regional PPOs in 2021.
Slightly more than half of all Medicare
Advantage enrollees would incur higher costs than beneficiaries in traditional
Medicare for a 6-day hospital stay
Medicare Advantage plans have the flexibility
to modify cost sharing for most services, subject to limitations. Total
Medicare Advantage cost sharing for Part A and B services cannot exceed cost
sharing for those services in traditional Medicare on an actuarially equivalent
basis. Further, Medicare Advantage plans may not charge enrollees higher cost
sharing than under traditional Medicare for certain specific services,
including chemotherapy, skilled nursing facility (SNF) care, and renal dialysis
services.
However, Medicare Advantage plans may reduce
cost sharing as a mandatory supplemental benefit, and may use rebate dollars to
do so. According to the Medicare Payment Advisory Commission (MedPAC), in 2021,
about 46 percent of rebate dollars were used to lower cost
sharing for Medicare services.
In the case of inpatient hospital stays,
Medicare Advantage plans generally do not impose the Part A deductible, but
often charge a daily copayment, beginning on day 1. Plans vary in the number of
days they impose a daily copayment for inpatient hospital care, and the amount
they charge per day. In contrast, under traditional Medicare, when
beneficiaries require an inpatient hospital stay, there is a deductible of $1,484 in 2021 (for one spell of illness) with
no copayments until day 60 of an inpatient stay (assuming no supplemental
coverage that covers some or all of the deductible).
In 2021, virtually all Medicare Advantage
enrollees (99%) would pay less than the traditional Medicare Part A hospital
deductible for an inpatient stay of 3 days, and these enrollees would pay $747
on average (Figure 3). But slightly more than half of all Medicare Advantage
enrollees (53%) would pay more than they would under traditional Medicare (with
its $1,484 deductible) for stays of 6 or more days, with average cost sharing
of $1,763, among those enrollees with costs above traditional Medicare.
For a stay of 10 days, 69% of Medicare
Advantage enrollees would pay more than beneficiaries in traditional Medicare,
and among those enrollees in plans with cost-sharing requirements that would
exceed the Part A deductible, average cost sharing would be $2,059. For a
length of stay of a least 20 days, 81% of Medicare Advantage enrollees would
pay more in cost sharing than the Part A deductible – $4,866 on average.
This analysis does not take into account the
fact that a majority of people in traditional Medicare would not pay the
deductible if hospitalized because they have supplemental coverage, although
those with Medigap or retiree health would have the additional cost of a
monthly premium. However, 5.6 million beneficiaries in traditional Medicare have no supplemental
coverage and would be liable for the full Part A deductible if
admitted to the hospital.
The average out-of-pocket limit for Medicare
Advantage enrollees is $5,091 for in-network services and $9,208 for both
in-network and out-of-network services (PPOs)
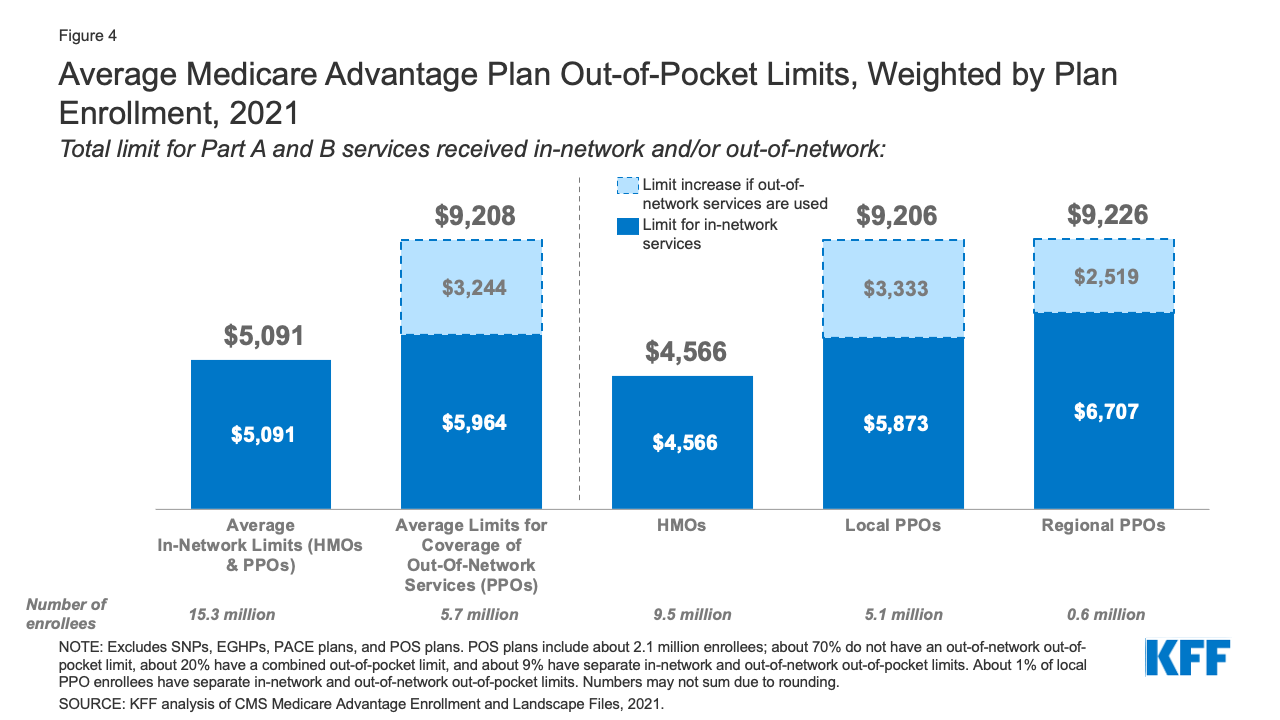
Figure 4: Average Medicare Advantage Plan
Out-of-Pocket Limits, Weighted by Plan Enrollment, 2021
Since 2011, federal regulation has required
Medicare Advantage plans to provide an out-of-pocket limit for services covered
under Parts A and B. In 2021, the out-of-pocket limit may not exceed $7,550 for
in-network services and $11,300 for in-network and out-of-network services
combined. These out-of-pocket limits apply to Part A and B services only, and
do not apply to Part D spending, for which there is a separate out-of-pocket threshold of $6,550 in 2021,
above which enrollees pay 5% of costs. Whether a plan has only an in-network
cap or a cap for in- and out-of-network services depends on the type of plan.
HMOs generally only cover services provided by in-network providers, whereas
PPOs also cover services delivered by out-of-network providers but charge enrollees
higher cost sharing for this care. The size of Medicare Advantage provider
networks for physicians and hospitals vary greatly both across counties and across
plans in the same county.
In 2021, the weighted average out-of-pocket
limit for Medicare Advantage enrollees is $5,091 for in-network services and
$9,208 for in-network and out-of-network services combined. For enrollees in
HMOs, the average out-of-pocket (in-network) limit is $4,566. Enrollees in HMOs
are generally responsible for 100% of costs incurred for out-of-network care.
However, HMO point of service (POS) plans allow out-of-network care for certain
services, though it typically costs more than in-network coverage. For local
and regional PPO enrollees, the average out-of-pocket limit for both in-network
and out-of-network services is $9,206, and $9,226, respectively.
The average out-of-pocket limit for in-network
services has generally trended down from 2017 but increased slightly between
2020 to 2021. The average in-network limit for HMOs increased from $4,925 in
2020 to $5,091 in 2021. The average combined in- and out-of-network limit for
PPOs increased from $8,828 in 2020 to $9,208 in 2021.
Most Medicare Advantage enrollees have access
to some benefits not covered by traditional Medicare in 2021 and special needs
plan (SNP) enrollees have greater access to certain benefits
Medicare Advantage plans may provide extra
(“supplemental”) benefits that are not available in traditional Medicare. The
cost of these benefits may be covered using rebate dollars (which may include
bonus payments) paid by CMS to private plans. In recent years, the rebate
portion of federal payments to Medicare Advantage plans has risen
rapidly, totaling $140 per enrollee per month in 2021, a 14% increase over 2020.
Plans can also charge additional premiums for such benefits. Beginning in 2019,
Medicare Advantage plans have been able to offer additional supplemental
benefits that were not offered in previous years. These supplemental benefits
must still be considered “primarily health related” but CMS expanded this
definition, so more items and services are available as supplemental benefits.
Most enrollees in individual Medicare
Advantage plans (those generally available to Medicare beneficiaries) are in
plans that provide access to eye exams and/or glasses (99%), telehealth
services (94%), dental care (94%), a fitness benefit (93%), and hearing
aids (93%). Similarly, most enrollees in SNPs are in plans that provide access
to these benefits. This analysis excludes employer-group health plans because
employer plans do not submit bids, and data on supplemental benefits may not be
reflective of what employer plans actually offer.
Though these benefits are widely available,
the scope of specific services varies. For example, a dental benefit may
include preventive services only, such as cleanings or x-rays, or more comprehensive
coverage, such as crowns or dentures. Plans also vary in terms of cost sharing
for various services and limits on the number of services covered per year and
many impose an annual dollar cap on the amount the plan will pay toward covered
services. Enrollees in SNPs have more access to certain benefits compared to
enrollees in individual plans, such as over the counter drug benefits (97% vs
79%); transportation (88% vs 37%); a meal benefit (73% vs 55%) and in-home
support services (14% vs 7%). However, there is no publicly available data on
how frequently supplemental benefits are utilized by enrollees or the amounts
they pay out-of-pocket for these services.
As of 2020, Medicare Advantage plans have been
allowed to include telehealth benefits as part of the basic benefit package
– beyond what was allowed under traditional Medicare prior to the public
health emergency. These benefits are considered “telehealth” in the
figure above, even though their cost may not be covered by either rebates or
supplemental premiums. Additionally, Medicare Advantage plans may also offer
supplemental telehealth benefits via remote access technologies and/or
telemonitoring services, which can be used for those services that do not meet
the requirements for coverage under traditional Medicare or the requirements
for additional telehealth benefits (such as the requirement of being covered by
Medicare Part B when provided in-person). The majority of enrollees in both
individual plans and SNPs have access to remote access technologies (70% and
79%, respectively), but just 5% of enrollees in individual plans and 6% of
enrollees in SNPs have access to telemonitoring services.
Nearly all Medicare Advantage enrollees are in
plans that require prior authorization for some services
Medicare Advantage plans can require enrollees
to receive prior authorization before a service will be covered, and nearly all
Medicare Advantage enrollees (99%) are in plans that require prior
authorization for some services in 2021. Prior authorization is most often
required for relatively expensive services, such as inpatient hospital stays,
Part B drugs, and skilled nursing facility stays, and is rarely required for
preventive services. Prior authorization is also required for the majority of
enrollees for some extra benefits (in plans that offer these benefits),
including comprehensive dental services, hearing and eye exams, and
transportation. The number of enrollees in plans that require prior
authorization for one or more services stayed the same from 2020 to 2021. In
contrast to Medicare Advantage plans, traditional Medicare does not generally
require prior authorization for services and does not require step therapy for
Part B drugs.
Discussion
In 2021, nearly two-thirds of Medicare
Advantage enrollees are in plans that do not charge a premium (other than the
Part B premium), although the remaining third do pay an additional premium,
averaging about $60 per month. Most enrollees are in plans that provide access
to a variety of supplemental benefits, such as eye exams, dental and fitness
benefits. Nearly all enrollees are in plans that require prior authorization
for some services. Medicare Advantage cost sharing varies across plans and can
be lower than traditional Medicare, but that is not always the case. Slightly
more than half of all Medicare Advantage enrollees would incur higher costs
than beneficiaries in traditional Medicare with no supplemental coverage for a
6-day hospital stay, though cost are generally lower in Medicare Advantage for
shorter stays.
While data on Medicare Advantage plan
availability and enrollment and plan offerings is robust, the same cannot be
said about service utilization and out-of-pocket spending patterns, which is essential
for assessing how well the program is meeting its goals in terms of value and
quality and to help Medicare beneficiaries compare coverage options. As
enrollment in Medicare Advantage and federal payments to private plans
continues to grow, this information will become increasingly important.
Meredith Freed, Jeannie Fuglesten Biniek, Tricia Neuman are with
KFF. Anthony Damico is an independent consultant.
|
Methods |
|
This analysis uses data from
the Centers for Medicare & Medicaid Services (CMS) Medicare Advantage
Enrollment, Benefit and Landscape files for the respective year. KFF is now
using the Medicare Enrollment Dashboard for enrollment data, from March of
each year. This analysis uses the term Medicare
Advantage to refer to Medicare Advantage plans and other types of private
plans, including cost and PACE plans. However, MMPs are excluded from this
analysis. Enrollment counts in publications by firms operating in the Medicare
Advantage market, such as company financial statements, might differ from KFF
estimates due to inclusion or exclusion of certain plan types, such as SNPs
or employer plans. For calculating how much Medicare
beneficiaries could pay out-of-pocket for an inpatient hospital admission, we
used the 2021 Medicare Plan Finder Benefit Summary data. For traditional
Medicare, beneficiaries without supplemental coverage would incur the Part A
hospital deductible of $1,484 in 2021 (for one spell of illness). For
Medicare Advantage, we use 2021 Medicare Plan Finder data to calculate
out-of-pocket costs for inpatient stays for Medicare Advantage enrollees,
weighted by 2021 plan enrollment. The analysis does not take into account
deductibles that some Medicare Advantage enrollees face, and if taken into
account, would increase costs for some enrollees. The analysis also does not
take into account maximum out-of-pocket limits under Medicare Advantage,
which would cap the amount enrollees pay for their care, including
hospitalizations. It is possible that some Medicare Advantage enrollees would
reach their out-of-pocket limit during their inpatient stay, particularly if
they had incurred high expenses prior to an inpatient admission. However, in
2021 the average out-of-pocket maximum is $5,091, which is above the
cost-sharing amount that all Medicare Advantage enrollees would pay for a
6-day hospital stay, assuming no other medical expenses during the coverage
year. |
No comments:
Post a Comment