Tara O'Neill Hayes, Margaret Barnhorst March 3, 2020
Executive Summary
·
Of the growing diabetic population in the United States, roughly
8.3 million people require insulin to regulate blood glucose levels, and it is
estimated that worldwide insulin use will increase 20 percent by the year 2030.
·
Competition in the insulin market has been limited for several
reasons: Products are not interchangeable, there are essentially only three
insulin manufacturers in the U.S. market, and no regulatory pathway has existed
to allow biosimilar products to create generic-like competition for insulin.
·
By the end of 2020, nearly all existing patents for insulin
products will have expired and a regulatory pathway for biosimilar insulin in
the United States will be available—changes that should facilitate downward
price pressure.
Introduction
Diabetes is a growing
health issue in America and is the seventh leading cause of death. Over 34.2
million Americans, or 10.5 percent of the U.S. population, had diabetes as of
2018.[1] Roughly 1.4
million Americans have type 1 diabetes, in which the body’s pancreas cannot
produce insulin on its own, usually a result of genetic abnormalities.[2] The remaining
majority of diabetics have type 2, in which the body cannot properly use the
insulin it has, often because of certain lifestyle factors. According to the
Centers for Disease Control and Prevention (CDC), another 84.1 million people
in America have prediabetes, a condition that if left untreated will lead to
type 2 diabetes within 5 years.[3] Gestational
diabetes occurs in roughly 14 percent of all pregnancies in the United States
and often goes away following delivery, but for nearly half of these women, it
will develop into type 2 diabetes within a few years following the pregnancy.[4]
Of the growing diabetic
population in America, nearly a quarter use insulin.[5] Insulin is a
necessary medication for nearly all type 1 diabetics (1.4 million people), and
roughly 21 percent of type 2 diabetics (6.9 million people) must also use
insulin to bring their blood glucose levels down to a healthy range.[6] Without
insulin, patients are likely to suffer from blurred vision, weight loss, and
intolerable thirst. Eventually, uncontrolled diabetes can lead to blindness,
kidney failure, gangrene, loss of limbs, and ultimately death.[7]
Insulin Manufacturers
and Products
There are 3 primary
insulin manufacturers in the U.S. market—Eli Lilly, Novo Nordisk, and
Sanofi—that represent over 90 percent of the global insulin market and produce
almost 100 percent of the insulin supply in the United States.[8] In general,
each manufacturer makes multiple types of insulin, and the only monopoly held
over one specific type is Novo Nordisk’s ultra-long-acting insulin.
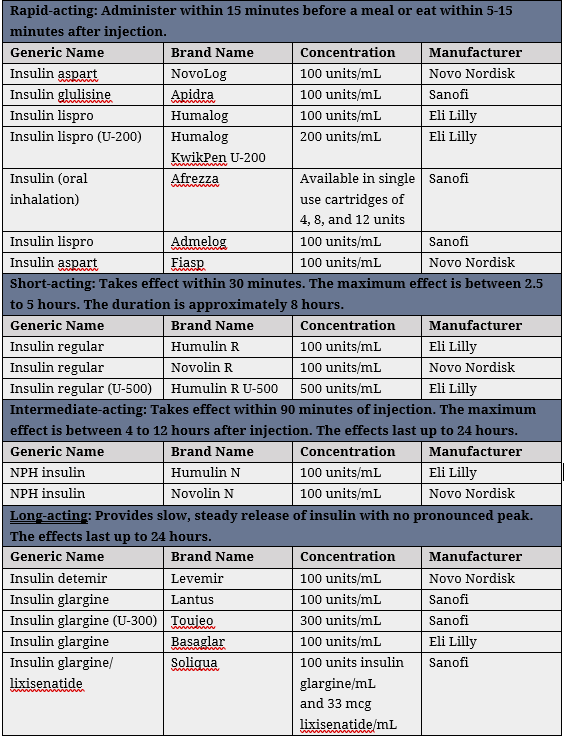

Source: Consumer Med
Safety[9]
Insulin was first
extracted from animals in 1923, but with technological advancements it was
synthetically manufactured from recombinant DNA in 1977 and called “human
insulin.”[10] There are
two types of insulin: basal and mealtime. Basal insulins may be either
intermediate or long-acting and help control insulin levels throughout the day.
Mealtime insulins are either short- or rapid-acting and, as the name
suggests, help control insulin levels around mealtime. Most people taking
insulin, particularly those with Type 1 diabetes, use both a basal and mealtime
insulin. There are also two types of active ingredients: human insulin and
insulin analogs. Insulin analogs are modified in laboratories and typically
provide better blood-sugar control than human insulin.[11] Also available is pre-mixed insulin,
which combines either fast- and long-acting insulins or short- and intermediate-acting
insulins, reducing the complexity and frequency of insulin administration.[12]
The improved blood
sugar control provided by analog insulin led to a dramatic shift in patient
use: In 2000, 96 percent of insulin users used human insulin and 19 percent
used analog insulin; by 2010, only 15 percent of patients used human insulin
while 92 percent used analog insulin.[13] Rapid-acting and ultra-long-acting
analogs are now the most widely prescribed types of insulin.[14]
There are several
other types of medications that people with Type 2 diabetes might take, besides
insulin, such as those listed here.[15]
Insulin
Administration
There are three
primary ways to administer insulin, and the most common is through injection.
There are now five types of injectable insulin that vary based on how quickly
they start working and how long they continue working—rapid-acting,
short-acting, intermediate-acting, long-acting, and ultra-long-acting.[16] Vials and
syringes are the cheapest way to inject insulin and the most widely used.
Insulin pens combine the vial and syringe in one product, providing greater
dose accuracy and easier administration, but for that reason they are often
more expensive than using a syringe.[17] Rapid-acting
insulin has the most diverse administration options available, including
syringe, pen, pump, or inhalation. Short-acting insulin can be administered
through a syringe, pen, or pump, while intermediate, long, and ultra-long
acting insulins can be administered only through a syringe or pen. Continuous
subcutaneous insulin infusion (CSII) devices, commonly known as insulin pumps,
are not manual injections but rather are battery-powered, computerized devices
programmed to deliver short-acting insulin under the skin continuously
throughout the day via a catheter attached to a person’s abdomen.[18] Insulin pumps are quite durable and can
last for years at a time, and therefore they are generally more expensive than
the supplies for manual injections.[19]
Another form of
insulin administration is infusion, where insulin is injected directly into a
vein through an IV. This is the preferred method to regulate blood glucose
levels for diabetic patients in hospital settings, for example during surgery,
labor and delivery, or in intensive care units.[20] The
prevalence of IV insulin administration in hospitalized settings is unknown,
but it is estimated that more than 20 percent of all adults discharged from
hospitals have diabetes.[21]
Inhaled insulin is a
relatively new form of insulin administration. Pfizer briefly introduced
Exubera in 2006 but then voluntarily withdrew it from the market within its
first year due to low sales.[22] In 2015,
Mannkind Corporation marketed Afrezza in the United States. Inhaled insulin is
rapid-acting and can be administered before meals to adults with type 1 or type
2 diabetes.[23] It is not a
replacement for long-acting insulin and typically must be used in combination
with injectable, long-acting insulin, meaning anyone using inhaled insulin is
likely also using another type of insulin.
Patient Choice
There is a pronounced
lack of choice for insulin regimens, and most of the choice that does exist is
left up to a physician or medical provider. Physicians recommend treatment
plans based on a person’s type of diabetes, lifestyle, and blood sugar levels
throughout the day.[24] Some people
only need one type of insulin, while others need multiple. For example, people
with type 1 diabetes generally need injections of long-acting insulin once or
twice a day, to mimic the body’s basal insulin, in addition to an injection of
rapid-acting insulin to cover mealtime spikes in blood glucose levels. People
with type 2 diabetes may only need long-acting insulin.[25] Patients are
generally able to choose their preferred method of insulin administration, when
the option is available, and they generally choose pens over syringes because
they are more convenient, easier to administer, and more easily transportable.[26]
Chemical differences
in insulin types and biological differences between diabetic patients make it
so that there is very little competition in the insulin market. Patients may
need to switch insulin plans for changes in blood sugar regulation, brand
availability, or hormones and metabolism due to aging. Because most insulin
products cannot substitute for each other, any changes must be prescribed or supervised
by a doctor.[27] The
variation between products and differences in individual blood sugar regulation
make switching from one type of insulin to another dangerous, and potentially
fatal, if not done correctly.[28] Furthermore,
for some people, switching from one type or brand of insulin to another has
caused allergic reactions with itching and swelling.[29] In short,
insulin is not a normal commodity.
Nevertheless, cost
considerations do come into play. Patients are more likely to follow and remain
on a prescription plan correctly if it is affordable, and as a result
physicians sometimes prescribe insulin plans that are the most cost-effective
for a patient, but not necessarily the best for that patient’s medical needs.[30]
Insulin Patents and
Market Exclusivity
Patents incentivize
the creation of new processes and products through two pathways: securing the
monetary gains from innovation by excluding others from using that invention
for a fixed amount of time, and then democratizing information. In the United
States, patent protections last for 20 years. Despite insulin being discovered
nearly 100 years ago, many insulin products still benefit from patent
protection. How can this be?
The insulin product
discovered in 1921 and patented in 1923 was extracted from animals.[31] In 1978, insulin was, for the first
time, reproduced from human recombinant DNA; this newly produced human insulin
was patented and brought to market in 1982. Several new analog insulin products
were developed between 1996 and 2005. The technological advances made over the
past century have allowed for improved purity, enhanced concentration,
increased supply, less crude extraction processes, easier administration, and
varying lengths of effectiveness (reducing the number of injections needed
daily) and quickness of onset, as discussed earlier.
Each time a company
invents a new or improved way to produce or administer insulin or changes how
long it lasts or how quickly it takes effect, it can receive a new patent.
Thus, while insulin itself may no longer be on patent—or at least not the early
insulin products brought to market—new insulin products (with, e.g., new
non-active ingredients), manufacturing processes, or administration devices may
be. As a result, there are currently hundreds of patents for insulin products.[32] A report
from the World Health Organization (WHO) in 2016 found that by 2020, more than
90 percent of all existing patents for insulin products will have expired
(excluding the patents on Pfizer’s inhaled insulin, which, as noted previously,
was pulled from the market).[33] Other companies have filed new patent
applications over the past several years, though, so the end of insulin patents
is still at least 20 years away.
The seemingly
constant stream of innovation does not mean, however, that patients have access
to older, and therefore cheaper, but still sufficient insulin products. When a
new product is brought to market, the older version is often either prescribed
less frequently or possibly even discontinued by the manufacturer.
Consequently, patients typically do not have access to many off-patent
insulins. In some instances, the new version may significantly improve patient
health and quality of life and is thus worth more to the patient, but sometimes
the improvements are minimal, and the price increase may exceed the added
value. WHO claims that not all inventions are, in fact, innovative, saying that
medical innovation should be measured in terms of added clinical value and
cost-effectiveness; not all newly patented insulin products meet this
definition of innovation, WHO argues.[34] Conversely, Doctors Jeremy Greene and
Kevin Riggs argue in the New England Journal of Medicine that “subsequent
iterations of insulin represented actual innovations, each one being safer,
more effective, or more convenient than its predecessor.”[35]
Besides patent
protections, the Food and Drug Administration (FDA) separately grants new drugs
periods of exclusivity of
varying lengths—meaning the product is protected in some way from direct
competitors. The length depends on the type of product and its approved uses. A
drug may receive a period of exclusivity even if it does not receive a patent.
Exclusivity refers to a period of time beginning upon the drug’s approval
during which a product effectively has exclusive rights to be sold in the U.S.
market. New biological products receive 4 years of filing exclusivity—during
which would-be biosimilar manufacturers are prohibited from filing an
application—and 12 years of approval exclusivity—during which the FDA is
prohibited from approving a biosimilar application.
Biosimilar Insulin?
The nature of insulin
itself has, to date, made it more difficult to generate effective market
competition. Insulin is a biological product (“biologic”)—the first,
in fact—though, when it was first approved by the FDA in 1982, it was
technically designated simply as a “drug” for regulatory purposes under Section
505 of the Federal Food, Drug, and Cosmetic (FD&C) Act.[36] Biologics are produced from material
from a living organism, not chemically synthesized molecules like most other
manufactured drugs.[37] Thus, even once the patents and
exclusivity periods expire, a competitor cannot make a generic version in the
traditional sense. Biologic products, by their nature, cannot be identically
duplicated, as is required for a product to be considered a generic; instead, a
manufacturer may make a biosimilar
product, whose molecular and biological structure shows no clinically
meaningful difference from the biologic.
From a regulatory
standpoint, however, there was not a legal pathway for biosimilars to come to
market until the Affordable Care Act (ACA) created one; the Biologics Price
Competition and Innovation Act included in the ACA created this pathway.
Section 7002 of the ACA also included a provision officially changing insulin’s
FDA designation (and all other biological products previously approved under Section 505
of the FD&C Act) from a “drug” to a biological product, as though it were
approved under Section 351
of the Public Health Service Act—a change that then allows for biosimilars.
This provision takes effect 10 years after the ACA’s enactment, allowing the
first biosimilar insulin to be approved on March 23, 2020.[38] Section 605
of the 2019 year-end government funding bill also included a provision amending
the definition of a biological product to now include any “chemically
synthesized polypeptide.” The FDA argues this addition is important to ensure a
biosimilar will also be able to come to market for any insulin that may be
manufactured as a chemically synthesized polypeptide in the future.[39]
Thus, while the U.S.
market has seen the introduction of a handful of follow-on insulin products
(and biosimilar insulin products are available in Europe),
there have not yet, technically, been any biosimilar insulin products in the
U.S. market.
Biosimilars should
lower the cost of insulin, but even with the new pathway competitors face
challenges. The follow-on products introduced to date did not have a dramatic
price-reducing effect, as was hoped, only reducing prices by about 10-15
percent.[40] (To be sure,
this result may be largely due to the fact that even these follow-on products
are manufactured by the three primary manufacturers rather than a competitor.[41]) Further, developing a biologic or a
biosimilar is much more complex and much more expensive than producing
small-chemical molecules, with the average cost an estimated 22 times greater
for a biologic product.[42] This cost
and complexity will likely slow the development of competitors in the insulin
market and prevent the kinds of price drops that have occurred with
small-molecule drugs.
Conclusion
Diabetes is one of the most burdensome
diseases in America, and about 1.5 million individuals are newly diagnosed with
diabetes each year. Soon, nearly 10 million Americans will need to take insulin
every day to live. Three manufacturers dominate the current insulin market, and
there is limited competition. That may soon change, however, as most patents
for insulin products will have expired by the end of this year, and biosimilar
insulin will finally be able to come to market. These factors may significantly
change the market for insulin—and thus the lives of millions of Americans who
depend on it.
[7] https://www.hopkinsmedicine.org/news/media/releases/why_people_with_diabetes_cant_buy_generic_insulin
[11] https://dtc.ucsf.edu/types-of-diabetes/type2/treatment-of-type-2-diabetes/medications-and-therapies/type-2-insulin-rx/types-of-insulin/insulin-analogs/
[12] https://dtc.ucsf.edu/types-of-diabetes/type2/treatment-of-type-2-diabetes/medications-and-therapies/type-2-insulin-rx/types-of-insulin/pre-mixed-insulin/
[16] https://www.diabetes.org/diabetes/medication-management/insulin-other-injectables/insulin-basics
[19]https://dtc.ucsf.edu/types-of-diabetes/type2/treatment-of-type-2-diabetes/medications-and-therapies/type-2-insulin-rx/insulin-administration/
[20] https://dtc.ucsf.edu/types-of-diabetes/type2/treatment-of-type-2-diabetes/medications-and-therapies/type-2-insulin-rx/insulin-administration/
[25] https://www.healthline.com/health/type-2-diabetes/basal-insulin/diabetes-statistics-and-basal-insulin-facts#3
[30]https://diabetescaucus-degette.house.gov/sites/diabetescaucus.house.gov/files/Congressional%20Diabetes%20Caucus%20Insulin%20Inquiry%20Whitepaper%20FINAL%20VERSION.pdf
[39] https://www.fda.gov/news-events/press-announcements/statement-low-cost-biosimilar-and-interchangeable-protein-products
https://www.americanactionforum.org/research/understanding-the-insulin-market/#ixzz6Fj7w7ZXQ
Follow @AAF on Twitter
Follow @AAF on Twitter
No comments:
Post a Comment