Tara O'Neill Hayes January 25, 2019
Executive Summary
- A Wall Street Journal report details
how private insurers that offer plans through Medicare Part D are
leveraging the program’s structure to contain their losses and increase
their profits, resulting in $9.1 billion in extra subsidies.
- Medicare Part D’s costs are rising for a number of
reasons, primarily as a result of an increase in spending in the
“catastrophic” phase of the insurance plans—the area of the program that
insurers are using to contain their losses.
- The
existing evidence on the program’s rising costs and misaligned incentives,
including the Journal’s report, demonstrates the importance of
restructuring the program to realign incentives for all stakeholders. One
such proposal is detailed here.
Introduction
A recent Wall Street Journal investigative
report made a dramatic claim in its headline: “The $9 Billion Upcharge—How Insurers Kept Extra Cash From
Medicare.” In this article, the Journal examines
how insurers set Medicare Part D premiums so as to increase the likelihood that
they will earn a profit on those plans at the expense of federal taxpayers.
The Medicare Part D program provides Medicare
beneficiaries with access to subsidized outpatient prescription drug coverage
through private insurance plans, and the program’s costs are rising. In 2018,
43.9 million seniors (or 73 percent of all Medicare beneficiaries) enrolled in
Part D, and enrollment—and therefore cost—is expected to increase each year for
the foreseeable future.[1] These
rising program costs have raised concerns among policymakers, and the Journal report
highlighted one area of concern: reinsurance.
The federal government covers most of the costs
in the final, “catastrophic” phase of Part D coverage—the reinsurance phase.
The recent exposé depicts insurers as exploiting the reinsurance structure to
guard against losses while using another aspect of the program’s structure—risk
corridors—to boost their profits illegitimately. Yet in structuring their plans
the way they are, insurers are legally and rationally responding to the
program’s incentives. To stop this practice and contain costs more broadly
within the Medicare Part D program requires reforms to the program’s structure.
One such reform option is outlined below.
Rising Reinsurance Costs
Overall program expenditures grew at an average
annual rate of 6 percent between 2007 and 2016, almost exclusively as a result
of rising reinsurance expenditures. The program’s rising reinsurance costs are
a function of both continued growth in the number of beneficiaries who reach
the catastrophic threshold as well as continued growth in the amount of
spending for each of those enrollees. Expenditures for such high-cost enrollees
rose at an annual rate of 10.4 percent between 2010 and 2015; in contrast,
average expenditures for the remainder of enrollees actually declined by an
average of 2.1 percent each year during that period.[2] Consequently,
spending above the catastrophic threshold has also been rising more rapidly
over this period relative to before 2010: 26.6 percent compared with 12 percent
previously.[3] Ultimately,
high-cost enrollees accounted for 57 percent of program expenditures in 2015,
despite being only 28 percent of beneficiaries.[4]
The growth in the cost of high-cost enrollees
not only increases the federal government’s cost to
subsidize the program, but also changes how the federal
government subsidizes the program. This rising spending has led to a dramatic
increase in the share of the federal government’s subsidy being paid through
reinsurance rather than premium subsidies: Reinsurance payments accounted for
less than one-third (31 percent) of the federal government’s share of the
program’s cost in 2007, but more than two-thirds of the cost in 2016 (68
percent).[5]
While the program has been largely successful, these and other trends over
the past several years have highlighted the need for structural reforms to
eliminate perverse incentives.
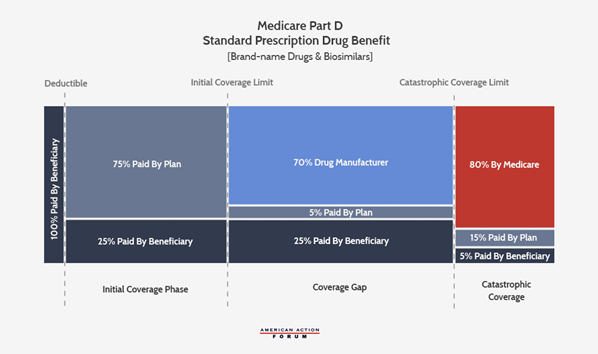
Understanding Medicare Part D’s Structure
Medicare Part D Bids
In order to participate in the program and
receive government subsidies for the coverage offered, Part D plan sponsors
(i.e. insurers) must submit a bid to the Centers for Medicare
& Medicaid Services (CMS) estimating their cost to provide the plan’s
covered benefits for each enrollee. Specifically, a sponsor’s bid reflects the
estimated cost of providing the “basic benefit” to an average beneficiary plus,
if it chooses, the estimated cost of any supplemental or enhanced benefits.[6] The
cost of the basic benefit is based on the plan’s required liability under each
phase of coverage, as shown in the chart below—including plans’ 15 percent
liability in the catastrophic phase.[7]
The Government Subsidy
The government subsidy has two components: the
direct subsidy of the premium and the reinsurance subsidy of excess
catastrophic costs. The direct subsidy covers 74.5 percent of the national
average bid for the basic benefit; it is paid to plans each month and does not
change throughout the year. Enrollees cover the difference between the direct
subsidy and the premium. If an enrollee chooses a plan with a
lower-than-average bid, they may not have to pay any premium, whereas enrollees
in plans with a higher-than-average bid will have to pay a larger premium.
If a plan’s costs for providing the basic
benefit are above or below their estimated costs, the direct subsidy payments
are reconciled with the plan’s actual costs at the end of the year—but only
under certain circumstances, as discussed below in the “Risk Corridors”
section. The circumstances create the room that insurers are using to make more
money, as the Journal reported.
The reinsurance subsidy covers 80 percent of
costs over the catastrophic coverage threshold beyond the amounts estimated in
the bid for the basic benefit. Unlike the direct subsidy, the reinsurance
subsidy is always reconciled with actual costs such that plans are protected
from ever having to pay more than 15 percent of each beneficiary’s catastrophic
costs.
The total government subsidy is supposed to
cover 74.5 percent of the program’s costs; however, this percentage is not set
in law.
Risk Corridors
When Congress and the Bush Administration were
creating Part D, there was concern among policymakers that few insurers would
offer plans because they would struggle to predict costs, and thus they would
face a substantial potential to lose money. Simply, if a plan’s actual costs
were more than expected, the direct subsidy payment would not cover as much of
their costs as intended; alternatively, if a plan’s actual costs were less than
estimated, the subsidy would be more than needed and the plan sponsor would
gain a profit. Accordingly, a risk corridor program was included to guard against
substantial financial losses while also preventing equally substantial profits
at the expense of beneficiaries and taxpayers.
The risk corridor established limits on both
financial gains and losses for a plan. If a plan’s actual costs for the basic
benefit are within five percent in either direction of the sponsor’s estimated
costs, there is no reconciliation of direct subsidy payments: The plan is
responsible for all the loss it incurs or may keep all of the additional
subsidy payments as profit. If a plan’s actual costs are more than 5 percent
but less than 10 percent above or below the sponsor’s bid, the first 5 percent
is treated the same, and the portion of loss or profit between 5 percent and 10
percent is split between the plan and Medicare 50/50. Similarly, if a plan’s
costs differ from the bid by more than 10 percent, the initial 10 percent is
treated as just described and the plan is responsible for 20 percent of the
losses over 10 percent if costs are higher than expected (or may keep 20
percent of the savings from the higher-than-needed direct subsidy payments over
10 percent). The following chart from the Medicare Payment Advisory Commission
(MedPAC) provides a helpful visual.[8]

The Impact: Why This Matters
Government Subsidy of Part D Increasingly
Consumed by Reinsurance
As noted, the growth in Part D spending is the
result of continued increases in both the number of high-cost enrollees and the
total amount spent for each of those high-cost enrollees. The program’s own
structure, however, has allowed for a third factor to increase program costs.
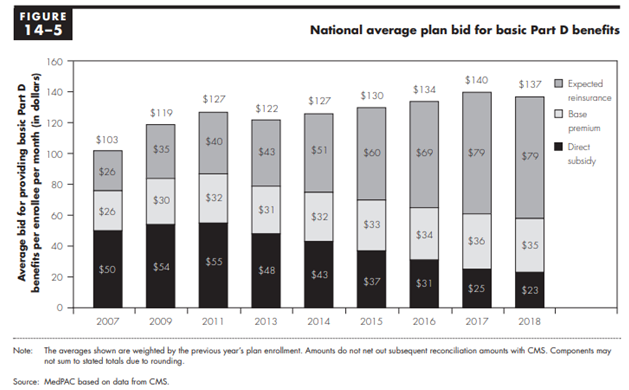
The federal government is supposed to cover 74.5
percent of all program costs (excluding beneficiary cost-sharing, Low-Income
Subsidy cost-sharing subsidies, and the coverage gap rebates), and that
percentage must be split between the direct premium subsidy, the additional
low-income premium subsidies, and the reinsurance costs. In order for this
percentage to remain fixed, the federal government’s direct premium subsidies
must decrease as reinsurance costs increase. This cost-shifting can be seen in
the following chart from MedPAC’s March 2018 Report to Congress, showing the
government’s declining direct subsidy of the premiums and increasing
reinsurance subsidies, as well as the base premium paid by beneficiaries.[9]
Because of the existence and nature of the risk
corridors along with the fact that this overall subsidy rate is not set in law,
the federal government has actually covered more than 74.5 percent of the
program’s costs in most years.[10] That
is, the structure and limited application of the risk corridors to the direct
subsidy payments allows plan sponsors to underestimate their catastrophic
coverage expenditures and be made whole for most of their additional costs,
while simultaneously overestimating their other expenditures without having to
pay back all of the excess premium subsidies. The result is that rising
catastrophic costs spill into rising overall program costs.
The Latest Findings
While MedPAC had previously noted the
possibility for plans to design their bids in such a way, they were unable to
find specific evidence of such behavior; MedPAC noted that to the extent such
behavior was occurring, it was likely limited. The Wall
Street Journal, however, found evidence that insurers were in fact using
these allowances to minimize the threat of financial losses and maximize gains.
Part D plan sponsors overestimated their basic benefit costs, and as a result
of the risk corridors they were able to keep an additional $9.1 billion beyond
what they would have if they had accurately estimated their costs.[11] On
the other hand, plan sponsors also underestimated their reinsurance costs by
$27.8 billion from 2006-2015, and Medicare reimbursed plans for all of these
additional costs.
The Need for Reform (And How to Do It)
In structuring their bids this way, the
insurers’ behavior is both fully legal and the rational result of the
incentives established by the program’s structure. If policymakers find this
behavior to be undesirable, they should change the program to eliminate the
incentives to behave this way.
One way to alter incentives would be to increase
plan sponsors’ liability in the catastrophic coverage phase. AAF has previously
proposed this and other comprehensive reforms of the Part D program. Those
proposals are detailed here. The aim of this proposal is to realign
the incentives of plan sponsors with those of the beneficiaries and taxpayers
in order to bring down program costs for all parties. This proposal includes
the introduction of a cap on beneficiary out-of-pocket costs, moving mandatory
drug manufacturer rebates to the catastrophic phase, and increasing insurers’
liability in the catastrophic phase while reducing the government’s reinsurance
liability.
CMS has also just proposed a new voluntary demonstration program for
the Part D program that attempts to address the issue of rising reinsurance
costs. Under this demo, Part D plan sponsors would take on increased liability
in the catastrophic coverage phase in exchange for the possibility of shared
savings. CMS would determine the expected expenditure rate absent the demo and
plans would be able to share in any savings below the expected expenditure
amount; plans would also be liable for additional costs if expenditures
exceeded the expected rate.
Current trends and projections, including the
drugs currently in development and their expected costs, all indicate that the
need for reform will continue to grow.
[1] https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/ReportsTrustFunds/Downloads/TR2018.pdf
[6] A risk adjustment program is used to
increase or decrease payments to plans based on an enrollee’s health to
mitigate any additional costs that may be incurred if enrollees are sicker than
average or vice versa.
[7] Plans may choose different benefit designs
with varying degrees of liability, but any variation must still be actuarially
equivalent to this standard benefit design.
[8] Chart from MedPAC June 2015 report, Chapter 6. Edited for
space, eliminating the visual of the structure of the risk corridors in 2006
and 2007.
[11] https://www.wsj.com/articles/the-9-billion-upcharge-how-insurers-kept-extra-cash-from-medicare-11546617082
https://www.americanactionforum.org/insight/evidence-for-structural-reform-part-d/#ixzz5ddAoDpTm
Follow @AAF on Twitter
No comments:
Post a Comment