What are
the social determinants of population health, and how can healthcare providers
reduce the socioeconomic impacts of community disparities?
Financially and
clinically successful population health management programs must take much more
into account than what happens to a patient while she is sitting on the exam
table.
As the healthcare system’s
responsibility expands beyond the clinic walls and into the community, the need
to understand and address the social determinants of health has
become a top priority.
Helping patients to
overcome socioeconomic barriers to better health by spending more on community
improvements can reduce downstream medical costs, found the Robert Wood Johnson
Foundation in a recent study.
States with a higher
ratio of social-to-healthcare spending from 2000 to 2009 saw better patient
outcomes.
A 20 percent increase
in the median social-to-health spending ratio was equivalent to 85,000 fewer
adults with obesity and more than 950,000 adults with mental illness, the study
added, significantly reducing the associated spending on these conditions and
their comorbidities.
But what are the most
impactful social determinants of health, how can providers identify areas of
opportunity in their communities, and how can they work with their partners to
reduce the negative impacts of socioeconomic insecurities?
The World Health
Organization defines social determinants as “the
conditions in which people are born, grow, work, live, and age, and the wider
set of forces and systems shaping the conditions of daily life.”
Economic and social
policies, political systems, and social norms all contribute to creating the
environments in which individuals thrive or experience challenges, WHO says,
leaving healthcare providers facing a complex and deeply personalized set of
restrictions and opportunities for each patient.
Few healthcare
organizations have the resources or political clout to truly eradicate the
larger economic, social, and historical constraints that have led to certain
groups experiencing long-term disparities and inequities.
But the good news is
that population health management programs that address small, manageable
pieces of the great American puzzle can successfully change many lives for the
better.
Breaking down the
social determinants of health into their component parts can help providers
assess their community challenges and implement targeted initiatives that
improve the health and wellbeing of patients experiencing socioeconomic
disadvantages.
SAFE AND
SECURE HOUSING
Housing stability is
a key indicator of socioeconomic status, affecting both rural and urban populations.
For most individuals, housing is the single greatest monthly expense, says the Johns Hopkins Center for
Health Equity.
Successfully making
rent or mortgage payments can be particularly difficult for low income
individuals who must spend a larger proportion of their earnings on securing
their housing situation.
Unstable housing
arrangements can increase emotional, physical, and social stress, present
problems with properly storing medications, make it difficult to consistently
access healthcare, and lead to gaps or changes in schooling for children that
may adversely affect their educational development.
Healthcare providers
can also more easily follow up with patients when they have a stable address
and contact information, Johns Hopkins adds.
Providers can work to
reduce the negative impacts of housing instability and homelessness by
partnering with supportive housing programs geared towards preventing loss of
housing and providing options for recently evicted or homeless individuals and
families.
The Department of
Housing and Urban Development offers grants to community
organizations looking to create supportive housing to supplement their efforts,
while the National Coalition for the Homeless maintains directories of existing supportive
housing projects, shelters, and transitional housing initiatives at the local
level.
ENGLISH
LANGUAGE PROFICIENCY AND CULTURAL UNDERSTANDING
Most healthcare in the
United States is conducted in English, despite the growing cultural diversity
that permeates the vast majority of communities. There are currently 41 million native
Spanish speakers in the country, in addition to 3.3 million people who speak
one or more dialects of Chinese.
Tagalog, Vietnamese,
Hindustani, Arabic, and Korean are also spoken by millions, leaving healthcare
providers with the task of ensuring that non-native English speakers can
understand directions and instructions that are often very complex, even for
those fluent in the language.
In 2004, more than 46 million people did
not speak English as a primary language, and 21 million additional residents
were not wholly fluent. By 2014, more than 60.6 million spoke a
language other than English at home.
These patients were
less likely than others to receive recommended preventive care, more likely to
struggle with their medications, and required more visits to the office to meet
their needs.
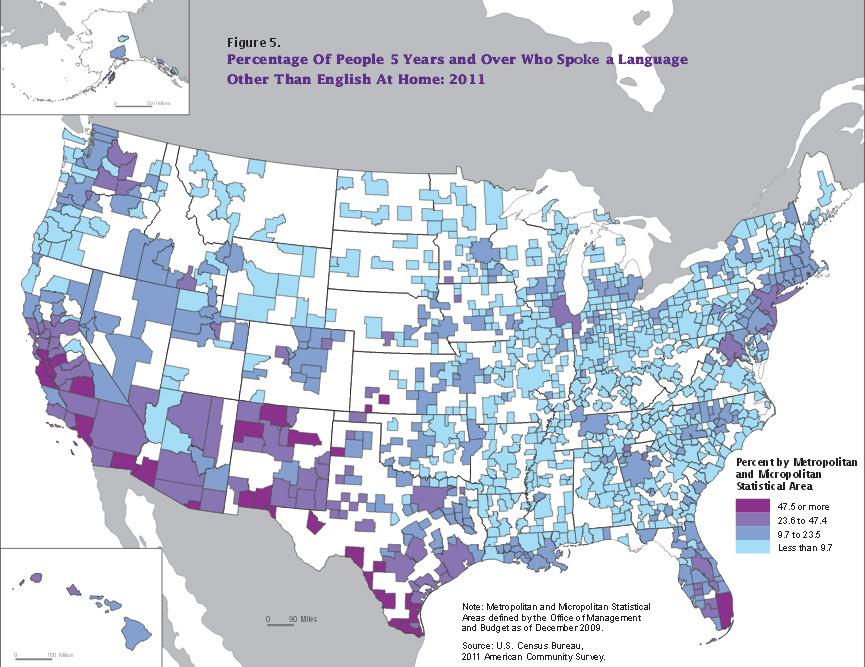
Source:
US Census Bureau
Interpreter services
can be costly, especially for uncommon languages. In 2004, the cost was
estimated at $279 per person per year. They also may not fully transcend
the cultural barriers experienced by non-native English speakers in the
healthcare setting.
And family members
who act as translators can increase tensions, reduce the feeling of
confidentiality, and present legal privacy concerns for providers, says Mayo
Clinic dermatologist Michael M. Wolz BMBCH, JD.
The advent of telehealth and mHealth translation services has
made it somewhat easier to overcome language barriers. On-demand
professionals with proficiency in uncommon languages can reduce the roughly $2
billion spent each year on interpretation services while ensuring access to
trained and certified healthcare-savvy translators.
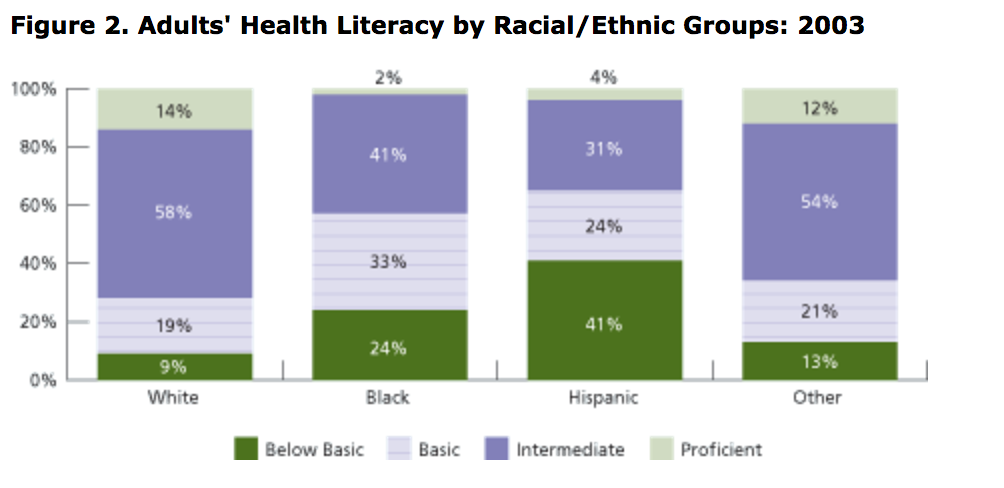
HEALTH
LITERACY AND EDUCATIONAL LEVEL
In addition to
ensuring that patients and providers are using the same words, organizations
must ensure that those words make sense to individuals with varying levels
of health literacy and educational
attainment.
Adults with higher
levels of education are less likely to engage in risky health behaviors, says AHRQ. And there are dramatic
differences in life expectancy strongly correlated with high school and college
graduation rates.
By age 25, adults
without a high school diploma are expected to die nine years earlier than their
graduate peers. Life expectancy among individuals with less than 12 years
of education has fallen by more than 3 years for men and 5 years for women
between 1990 and 2008.
Source:
US Dept. of Education
Educational
attainment is correlated with higher incomes,
more social resources and stability, improved healthy behaviors, and an
improved ability to tackle social and economic stresses. Individuals who
secure stable employment are more likely to live in neighborhoods with access
to fresh food choices, higher quality schools for their children, and lower rates
of violence and crime.
High school graduates
are also less likely to be obese, to use
tobacco, to be uninsured, to access preventive care and cancer screenings, and
to exercise an appropriate amount, the CDC notes.
The “soft skills”
learned in school, such as critical thinking, reading comprehension, and social
interactions, also contribute to higher levels of health literacy.
Health literacy
allows patients to understand their conditions and the treatments that will
improve their overall wellbeing, yet only 12 percent of adults are “proficient”
in the art of understanding their health, according to the National Assessment
of Adult Literacy.
Providers can help to
develop health literacy in patients, no matter what degrees they hold, by
training their clinicians in how to communicate clearly and effectively while
reducing stress and defensive anxiety in the consult room.
Treating individuals
with kindness, patience, and respect while
using simple language to explain health issues can help to ensure communication
is achieved.
TRANSPORTATION
ACCESS
If patients cannot
physically get to their appointments or access acute care in times of need,
they cannot benefit from even the most robust and effective population health
management program.
Missed appointments
and no-shows cost the healthcare system billions of dollars each
year. One estimate from 2008 says the
average cost of no-shows per patient was nearly $200. With a mean no-show
rate of close to 20 percent in an average clinic, providers have a significant
financial incentive to improve these figures.
Transportation
problems are only one small part of the reason why patients might skip out on
their scheduled visits, but ensuring access to a lift is one of the easier
issues to address.
Medicaid provides non-emergency transportation
services to beneficiaries who do not have access to – or cannot utilize – cars,
trains, or buses to get to their medical appointments. Beneficiaries who
do not hold a driver’s license, don’t have a working vehicle in the household,
or have a disability or condition that precludes independent travel are
eligible for covered transportation services.
The advent of
ridesharing services has also revolutionized the routine healthcare transport
environment. In 2016, a study published in the Journal of
the American Medical Association estimated that ridesharing apps like Lyft and
Uber could significant reduce the $2.7 billion federal spend on non-emergency
transportation.
Industry partnerships
have proliferated rapidly, allowing patients to
access services through their smartphones at lower costs to the healthcare
system. As these companies continue to expand into more cities and rural
areas, patients may be less likely to miss their scheduled visits.
The CDC also provides
a transportation health impact assessment toolkit for
providers who wish to understand their community’s challenges and implement
strategies to reduce burdens and improve mobility.
ACCESS TO
HEALTHY, NUTRITIOUS FOOD CHOICES
Dietary choices are
directly linked to the development of costly chronic diseases such as diabetes
and cardiovascular conditions. Access to healthy, safe, and produce-rich
food choices can reduce malnutrition and its associated risk of
infectious disease as well as the economic burdens of obesity, which were estimated at $147 billion in
2008.
In 2012, the costs of
diabetes totaled $245 billion, including $176 billion in direct healthcare
costs and around $69 billion in productivity losses.
Just over half of US
residents adhered to recommended dietary guidelines in 2010, while only 20
percent of adults received the recommended amount of daily physical activity
each day.

Source:
CDC
About three-quarters
of the population fails to incorporate enough fruits and vegetables in their
daily diets, and most exceed the recommended levels of
fats, sugars, simple carbohydrates, and sodium.
Educating patients
about their dietary habits is an important component of improving eating
habits, but so is ensuring that individuals can access affordable healthy foods
easily within their communities.
Nearly 30 million people live in areas where
the closes grocery store offering produce and other fresh options is more than
a mile away. In rural areas, the closest supermarket is often 20 miles
away or more. For residents with limited transportation options, this is often
too far – especially when convenience stores and fast-food outlets offer closer,
cheaper options for a quick meal.
The Healthy
Food Access Portal, supported by a collaborative partnership
including the Robert Woods Johnson Foundation and Center for Healthy Food
Access, can help providers engage in federal and local-level policy initiatives
geared at expanding access to quality food choices in low-income and
underserved communities.
PUBLIC
SAFETY AND INTERPERSONAL VIOLENCE
Communities with high
levels of crime and violence are also among the most likely to experience
widespread economic and social instability. High rates of incarceration,
the threat of domestic abuse, child abuse, and interpersonal violence, and
prevalent street crime can lead to significant difficulties with maintaining
healthy behaviors and accessing care.
Homicide takes more
than 16,000 lives each year, and is the leading cause of
death for people aged 15 to 24. In 2011, six percent of high school-aged
youths said they skipped at least one day of school in a 30-day period due to
feeling too unsafe to attend.

Source:
FBI / FactCheck.org
Violence can also
easily spill over into the healthcare setting, putting clinicians and other
staff members at risk. Healthcare organizations spend around $2.7 billion
each year on proactive and reactive violence response efforts, the American
Hospital Association said in a 2017 report.
The figure includes
$280 million for preparedness and prevention, $852 million in uncompensated
care for victims of violence, more than $1 billion on training to prevent
violence in hospitals, and $429 million coping with care, indemnity, and other
costs resulting from violence against hospital employees.
The American Society
for Healthcare Risk Management provides a healthcare facility workplace violence
assessment toolkit that can help organizations
reduce their incidence of violence against staff.
Addressing violence
in the community and between individuals requires a concerted, policy-based
approach to eliminating opportunities for violence,
reducing income inequality that leads to violent tensions, and ensuring that
victims of abuse and violence have the resources, support, and skills they
need to leave dangerous situations.
SOCIAL
SUPPORT AND CAREGIVER AVAILABILITY
Loneliness is one of
the biggest and most underreported public health threats. While seniors
are prone to feeling isolated as their social connections change with age,
children and teenagers are also extremely likely to feel as if they are unable
to share their emotions and thoughts with friends or family.
The stress of social
isolation can lead to premature cognitive
decline and dementia, increased risk of cardiovascular disease, exasperation of
depression and anxiety, and premature death.
Strong social support
networks for children and adolescents contribute
to building mental and emotional resiliency that may help to reduce the
likelihood of engaging in risk behaviors, succumbing to peer pressure, or
developing anxiety-driven behavioral health concerns.
For seniors,
caregivers are often involved in making critical health decisions and helping
elderly patients cope with hospitalizations and declining independence. About
half of elderly patients require significant help with decision-making when
hospitalized, said a 2014 study from JAMA.
Nearly 60 percent of the
decisions made by caregivers in these situations involved life-sustaining care,
while half involved discharge planning and post-acute care.
While the
availability of caregivers is crucial for many patients, healthcare providers
must also provide support for family members and friends charged with the
difficult task of overseeing the needs of their loved ones.
Stress, anxiety, and
depression among caregivers are extraordinarily prevalent, with some
estimates showing that between 40 and 70
percent of caregivers experience clinically significant mental health
concerns. As patients decline in health, the mental health impacts on
their caregivers increase dramatically as feelings of frustration, helplessness,
loneliness, grief, and guilt can rise.
Ensuring that both
patients and their caregivers have the emotional and social support required to
make the best possible decisions for themselves and their loved ones can help
to reduce the negative impacts of many social determinants of health.
Robust social support
networks and community initiatives can prevent malnutrition and improve social interactions among
seniors, lower the risk of adolescents engaging in interpersonal violence or
leaving school, reduce the risk of chronic disease development due to stress,
and make it easier for caregivers to maintain stable employment as well as
their own friendships and relationships while they make informed decisions
about care.
Successful population
health management programs that hope to address the myriad social determinants
of health – including the many factors not directly outlined here – will be
rooted in providing compassionate, holistic, and personalized support to
individuals facing any number of socioeconomic challenges and obstacles in
their daily lives.
This article was
originally published on August 18, 2017.
https://healthitanalytics.com/features/what-are-the-social-determinants-of-population-health?eid=CXTEL000000460294&elqCampaignId=8190&elqTrackId=ddce3d9e6a0a4d6d90ae18db36f46bbc&elq=03800397e0fc4aa9a067e9ae4b051f95&elqaid=8638&elqat=1&elqCampaignId=8190
No comments:
Post a Comment