Tara O'Neill Hayes September 23, 2019
Executive
Summary
In the
past few months, Congress has put forward several proposals to lower prescription drug
costs. One proposal considered and approved by the Senate Finance Committee
(Finance) is the Prescription Drug Pricing Reduction Act (PDPRA) of 2019.
Among its several provisions, this legislation included
a redesign of the Medicare Part D Prescription Drug Program, similar to the American Action Forum (AAF) proposal from
August 2018. Speaker
Pelosi recently released another drug pricing reform package that
also included an alternative proposal to redesign the Part D benefit structure.
This paper analyzes those two proposals relative to current law and the AAF
proposal.
·
All of the pending proposals seek to put downward pressure on
prescription drug prices by realigning incentives in the Medicare Part D
program, specifically by requiring manufacturer rebates (at least) in the
catastrophic phase of the benefit rather than the coverage gap. Shifting the discount
to this phase ensures the mandatory discount increases along with a drug’s
price.
·
While the plans are conceptually similar, the varying parameters
of the proposals result in significantly different impacts for the various
stakeholders, with both the Finance and Pelosi proposals increasing drug
manufacturer liability to an unprecedented level.
·
This study analyzes how these plans would be expected to impact
spending in 2022, looking just at those drugs for which annual spending is high
enough to require a rebate payment if a beneficiary took only that drug. Under
the AAF proposal, it is estimated that drug manufacturers would pay a minimum
of $4.1 billion in rebates on such drugs in 2022. The Finance proposal would
yield an estimated $8.4 billion in rebates from those drugs. The Pelosi plan
would result in $23.1 billion in rebates.
Comparing
the Proposals to Reform Medicare Part D
The
current structure of Medicare Part D has several notable problems. Because insurer
liability is now quite limited beyond the deductible, insurers have little
incentive to keep beneficiaries out of the coverage gap and catastrophic
phases. Further, drug manufacturers lack strong incentives to keep their prices
down. The result of this lack of incentives is that the government is paying an
increasing share of Part D’s cost in the catastrophic phase, and the
government’s overall costs are rising. Finally, the current structure leaves
some beneficiaries with very high costs even in the catastrophic phase. The
American Action Forum (AAF) proposal illustrates how benefits can be
restructured to realign incentives and market forces employed to put downward
pressure on prices.
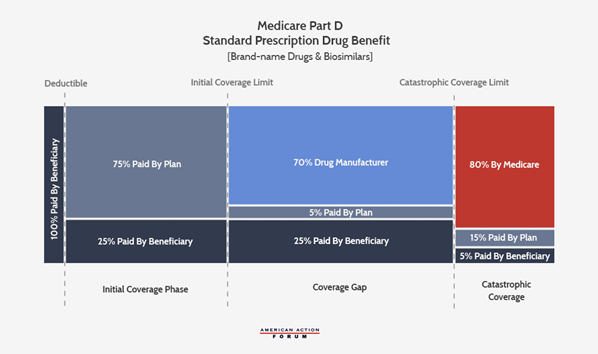
Current Law
The
following graphic illustrates the current Part D benefit structure. Most
recently reformed in 2018, drug manufacturers now pay 70 percent of costs in
the coverage gap while insurers pay just 5 percent during that phase. The
federal government covers 80 percent of costs in the catastrophic phase and
beneficiaries pay 5 percent of catastrophic costs, with no out-of-pocket (OOP)
cap.
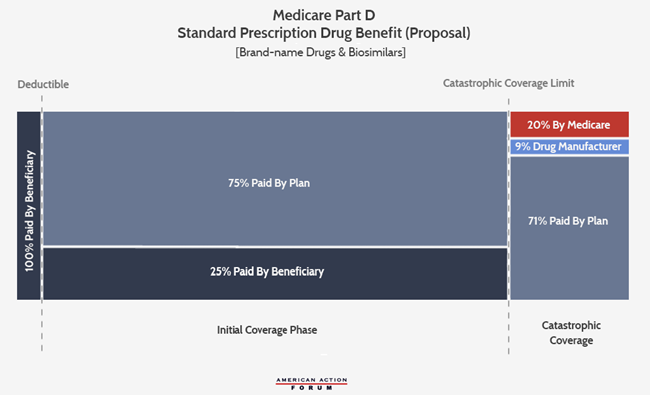
AAF
Proposal
The AAF proposal addresses the aforementioned problems
by making several changes, shown below: It increases insurer liability in the
catastrophic phase, moves the required manufacturer rebates to the catastrophic
phase, and places a cap on beneficiaries’ OOP liability. The accounting firm Milliman modeled this plan and current law to
find the parameters at which the expected manufacturer rebates under this
proposal would be equal to what is expected under current law from 2020-2029.
It estimated that an OOP cap of $2,500 would yield manufacturer rebates roughly
equal to current law if manufacturers paid a 9 percent discount in the catastrophic
phase for all beneficiaries.[i]
Following MedPAC’s lead, the AAF proposal sets the
government’s reinsurance liability at 20 percent, leaving insurers liable for
71 percent of costs in the catastrophic phase.
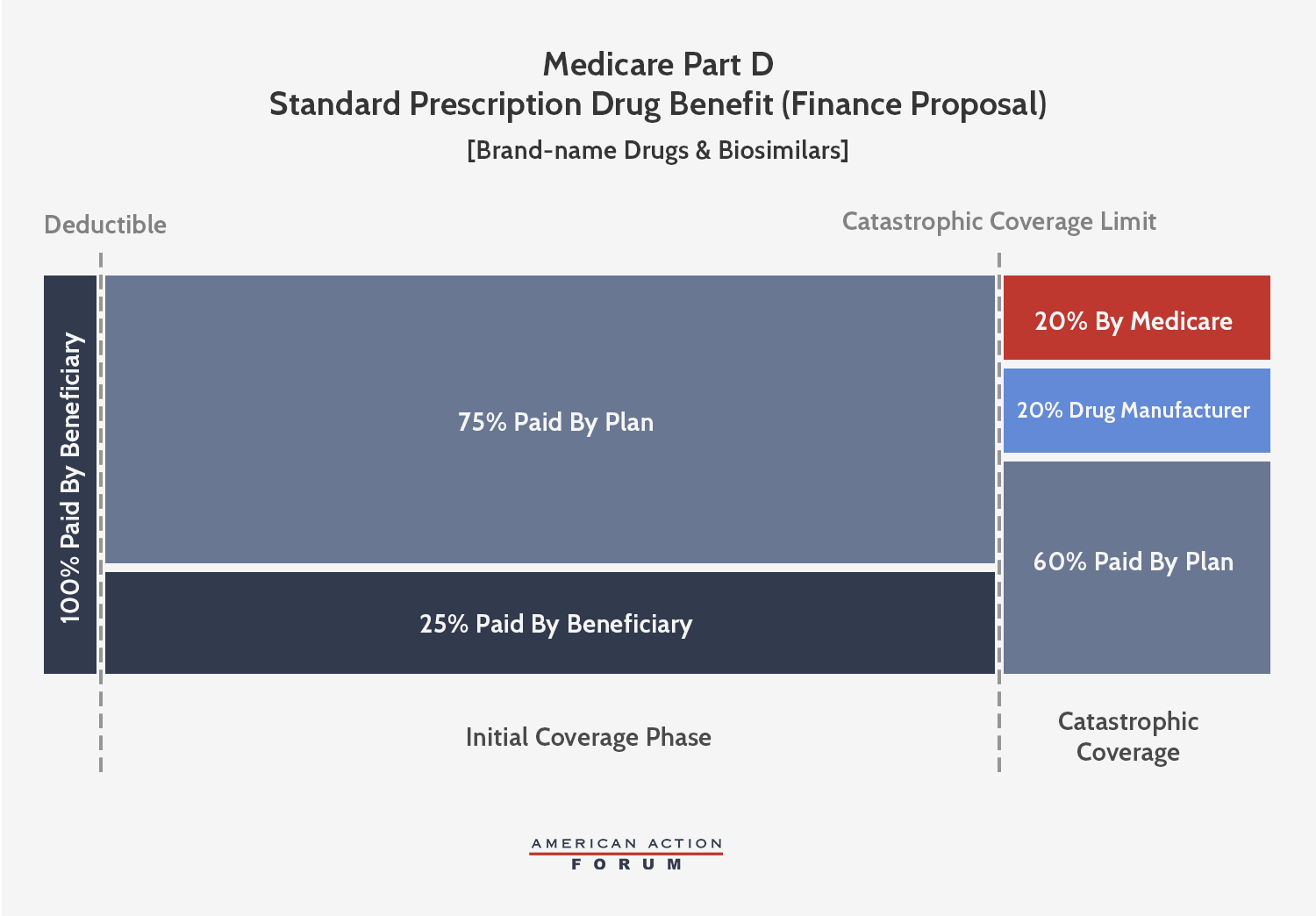
Senate
Finance Proposal
The
Senate Finance Committee’s (Finance) Prescription Drug Pricing Reduction Act (PDPRA) of 2019
includes a similar conceptual framework to the AAF proposal, but the OOP limit
and the catastrophic phase liabilities are different. The Finance proposal,
which would be phased-in beginning in 2022, sets an OOP limit of $3,100, equal
to the amount of OOP spending before the catastrophic threshold expected under
current law. The proposal would require brand-name and biosimilar drug
manufacturers to pay a 20 percent rebate for all drug costs incurred after the
beneficiary reaches the catastrophic phase, more than double what AAF proposed.
Insurer liability in the catastrophic phase would gradually increase to 60
percent by 2024. Federal reinsurance would be reduced to 20 percent for
brand-name drugs and biosimilars and 40 percent for generic drugs by 2024.
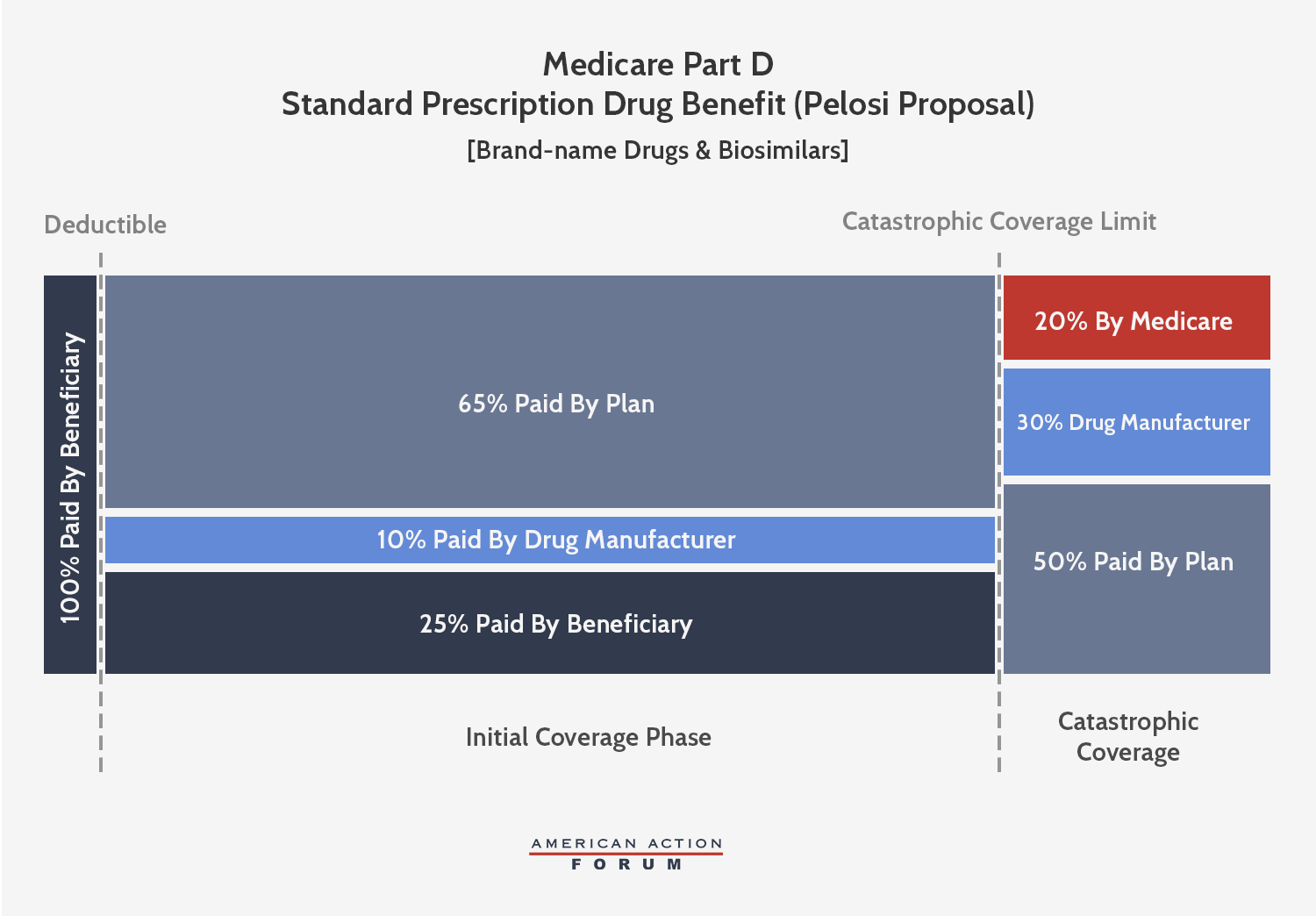
Pelosi
Proposal
Speaker Pelosi’s
proposal is also conceptually similar to the AAF proposal, but, like
the Finance proposal, sets different parameters that extract even more money
from manufacturers. This plan would cap beneficiary OOP spending at
$2,000—about $600 less than what a beneficiary reaching catastrophic coverage
pays in 2019. Brand-name and biosimilar drug manufacturers would be
required to pay a 30 percent discount for all drug costs incurred after the
beneficiary reaches the catastrophic phase, more than triple what AAF proposed.
Further, manufacturers would be required to pay 10 percent of costs in the
initial coverage phase, as well, meaning rebates will be required for all drugs
taken after a beneficiary reaches the deductible. Insurer liability in the
initial coverage phase would thereby be reduced to 65 percent when a
beneficiary takes a brand-name drug or biosimilar. In the catastrophic phase,
insurer liability would increase to 50 percent for brand-name drugs and
biosimilars and 80 percent for generic drugs, while federal reinsurance would
cover the remaining 20 percent.
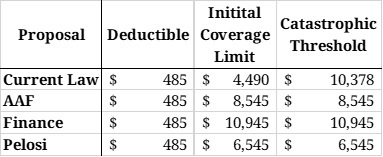
As you
can see in Table 1, all three proposals would eliminate the coverage gap that
currently exists, reducing the number of coverage phases to three.
Table 1:
Coverage Phase Thresholds
Estimating
the Impact
The
Maximum Rebate Per Drug
Under
each proposal, the required rebate amount for a given drug can be calculated
based on the drug’s price. As shown in the second and third columns of Table 3,
the current coverage gap rebate shrinks proportionately as the price of the
drug increases because the rebate amount is capped indirectly. For example, a
drug costing $10,378 (the lowest cost at which the maximum rebate
must be paid) pays a rebate equal to nearly 40 percent of the cost of the drug.
A drug priced at $55,000, on the other hand, pays the same rebate amount, but
that amount is equal to only 7.5 percent of the drug’s price. Thus, the current
benefit design is more harmful to lower-priced drugs. If the rebate were
required in the catastrophic phase of coverage, however, it would no longer be
capped, and the required rebate amount would increase, both nominally and as a
share of the drug’s price, as the price increases, as shown under each of the
proposals. As a result, more of the burden of the rebates would be placed on
the higher-priced drugs, as shown by the various proposals.
Table 3:
Rebates Required Under Various Reform Proposals
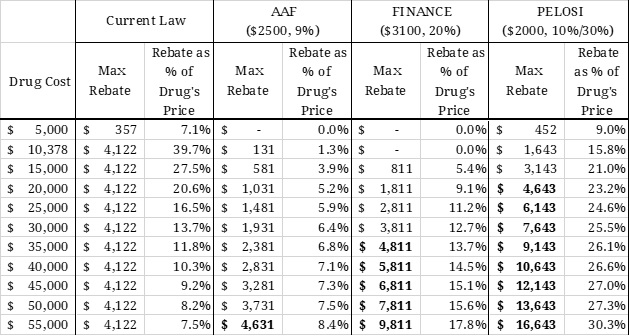
Stakeholder
Liability and Total Rebates CollectedRebates under the Finance proposal would be more than double the
rebate required by the AAF proposal. The Pelosi proposal will require rebates
that are 3.6 times the amount required by the AAF proposal. The bolded numbers
indicate the “break-even price” (at which point the rebate
amount required under the proposals is equal to the currently required rebate
amount). This price would be significantly lower under the Finance proposal,
and lower still under the Pelosi proposal, than the break-even price for the
AAF proposal. The break-even price under AAF’s proposal in 2022 is $54,342. In
other words, manufacturers would spend the same amount on rebates much more
quickly under the Finance or Pelosi proposal than under the AAF proposal.
Next,
using spending and utilization data from 2017 provided in the CMS Medicare Part D Drug Spending Dashboard,
AAF estimates some of the expected costs to the various stakeholders in
2022—the first year that these proposals would be implemented. Only drugs for
which estimated average annual per beneficiary spending exceeds the threshold
at which a rebate would be required is included in the estimate of total
rebates that must be paid; thus, these estimates represent the low-end of the
amount likely to be collected. Additional assumptions and limitations are
explained in the appendix.
Table 4:
Liability Before the Catastrophic Phase
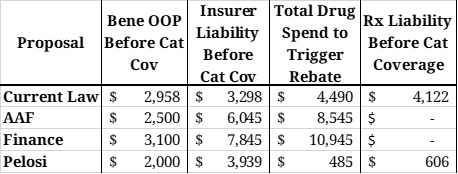
Table 4
illustrates various stakeholder liabilities and relevant spending thresholds on
an individual level, assuming a beneficiary incurs enough costs to reach
catastrophic coverage taking only brand-name drugs and/or biosimilars. Under
all reform proposals, beneficiaries would not owe anything more once they reach
the catastrophic phase; under current law, beneficiaries must continue to pay 5
percent of all costs in the catastrophic phase. OOP spending before the
catastrophic phase would be closest to that expected under current law in the
Finance proposal. Insurer liability before the catastrophic phase, shown in
Column 3, would be closest to current law liabilities under the Pelosi
proposal.
Column 4
is the amount of total drug spending that must be incurred before a drug
manufacturer is required to pay a rebate. Under current law, rebates are
required in the coverage gap; under the Pelosi proposal, rebates would be
required once a beneficiary reaches their deductible. Under the AAF and Finance
proposals, rebates would not be required until the beneficiary reaches
catastrophic coverage. As shown in the last column, the minimum amount of total
drug spending that must be incurred to reach the catastrophic phase is lowest
under the Pelosi proposal, followed by the AAF proposal; the Finance proposal
would require slightly more spending than current law.
Table 5:
Liability in the Catastrophic Phase with $30,000 in Drug Costs
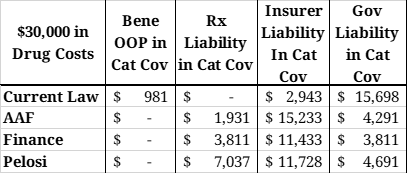
Table 5
shows the costs that would be covered by each stakeholder in the catastrophic
phase for a beneficiary with $30,000 in brand-name or biosimilar drug costs.
The chart below illustrates total costs by payer for the same scenario. Each
proposal will significantly reduce government liability. Total manufacturer
liability is smallest under the AAF proposal and largest under the Pelosi
proposal. Insurer liability is most limited under current law and highest under
the AAF proposal.
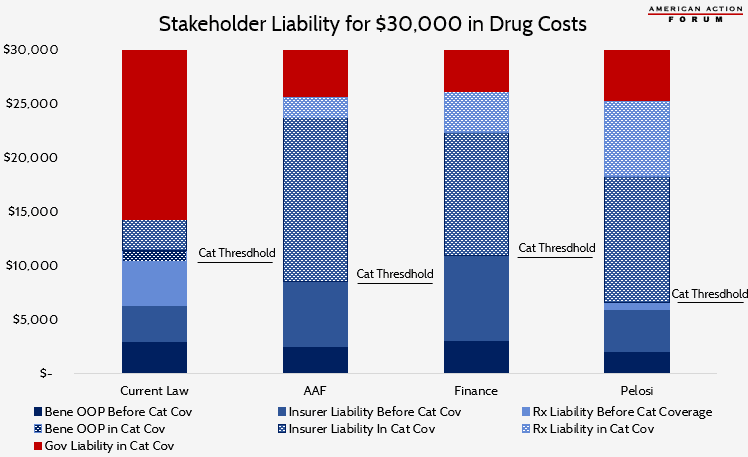
Table 6:
Required Rebates
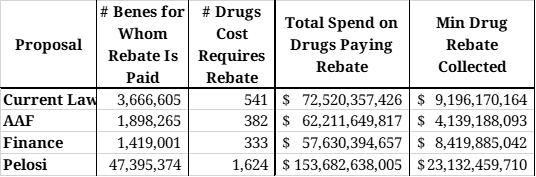
Table 6
illustrates the number of drugs and beneficiaries for which a rebate will be
required under each of the plans, as well as the expected total rebates to be
collected for those drugs.
Under the
AAF proposal, an estimated 382 drugs would have an average cost per beneficiary
exceeding $8,545 in 2022 and will be provided to nearly 1.9 million
beneficiaries at a total cost of $62.2 billion. Spending above the catastrophic
threshold for these drugs will equal an estimated $46.0 billion. If a 9 percent
rebate were required from drug manufacturers for all spending in the
catastrophic phase, $4.1 billion in rebates would be collected on these drugs
alone in 2022. Given that modeling found this rate would provide roughly
equivalent rebate collections as current law, and it is estimated that $9.2
billion in rebates would be collected under current law, more than half of the
rebates collected under the AAF proposal would be paid for drugs costing less
than $8,545, and are not included in this estimate.
For the
Finance proposal, it is estimated that the manufacturers of 333 drugs provided
to 1.4 million beneficiaries will be required to pay a rebate based on their
cost alone. Spending above the catastrophic threshold for these drugs will
equal an estimated $42.1 billion. A 20 percent rebate in the catastrophic phase
would yield $8.4 billion in rebates on just these drugs in 2022. Similar to the
AAF proposal, it is likely that half of expected rebates will be paid for drugs
costing less than $10,945, and thus are not accounted for in this estimate.
The
Pelosi proposal would impact exponentially more drugs because rebates will be
required after just $485 in spending. An estimated 1,624 drugs provided to 47.4
million seniors would trigger the initial rebate threshold. Total spending on
these drugs is estimated at $153.7 billion in 2022. Requiring manufacturers to
pay 10 percent of costs incurred between the deductible and the catastrophic
phase will yield an estimated $8.0 billion in rebates. Nearly one-fourth of
those drugs (428), provided to an estimated 2.4 million beneficiaries, are also
expected to trigger the catastrophic threshold rebate, which would result in
$15.1 billion in discounts. Thus, manufacturer liability under the Pelosi
proposal would total an estimated $23.1 billion in 2022. Because most drugs
would trigger the rebate requirement on their own, this estimate likely
captures most of the total rebates that would be collected under Pelosi’s plan.
Based on this estimate, drug manufacturers would be required to pay roughly 12
percent of the program’s total costs.
Beneficiary
OOP Costs
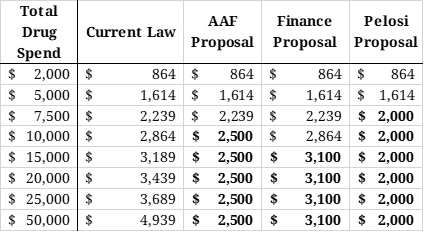
The last
table shows the various OOP requirements that would be required of
beneficiaries under current law as well as the various proposals at various
total drug costs. Under the AAF proposal, beneficiaries would benefit from the
$2,500 OOP cap after $8,545 in total drug costs. Under the Finance proposal, the $3,100 OOP cap would not
reduce beneficiaries’ OOP liability, relative to current law, until total drug spending
surpassed $10,945 in total drug costs. Under the Pelosi proposal, beneficiaries
would begin to see OOP savings after just $6,545 in total drug costs.
Table 7:
Out-of-Pocket Requirements Under Various Proposals
Implications
The AAF
proposal was designed, not to extract additional funds from the pharmaceutical
industry, but rather to create natural market pressures to control costs. The
Finance and Pelosi proposals, on the other hand, will require significantly
larger discounts from the pharmaceutical industry. The discount rates may be
large enough to actually be detrimental to the industry and may result in reduced investment for future innovation. And
that is to say nothing of the numerous other hits to the industry included in
other sections of each of the bills, as discussed here and here.
The
impact to beneficiaries depends on two primary components: any change in OOP
costs and the change in premiums. High-cost beneficiaries who are expected to
reach the catastrophic phase under current law will certainly benefit from
lower OOP costs under either the AAF or Pelosi proposals and will very likely
benefit from the Finance proposal. The Milliman analysis of the AAF proposal
estimates that beneficiaries would save up to $41.3 billion in OOP costs from
2020-2029. A preliminary estimate of the Finance proposal
from the Congressional Budget Office found that beneficiaries would save $20
billion in OOP costs as a result of the redesign. Beneficiaries with lower
costs may be worse off under these proposals, as they may experience higher
premiums without the benefit of reduced OOP costs.
Higher
premiums, however, would be indicative of a better functioning insurance
program. Premiums reflect expected insurer liability. The premise of these
plans, in part, is that increasing insurer liability will increase their
incentive to control costs. The proposals also aim to reduce OOP expenses for
those with the highest costs; doing so typically requires shifting costs to the
insurer, though, in Part D, the government and drug manufacturers also pay some
of the costs. To the degree that insurer liability rises, premiums will
necessarily rise proportionately. Because insurer liability is expected to be
lowest under the Pelosi proposal, premiums would likely be lowest under her
plan, including relative to current law. This is despite setting the lowest OOP
cap, because her plan shifts significantly more liability to the drug
manufacturers. CBO found that premiums would likely be reduced by just less
than $1 billion under the Finance proposal,
relative to current law, as a result of the redesign (plus another $5 billion
reduction associated with inflation rebate penalties). Premiums would likely be
highest under the AAF proposal where insurers would have the greatest
liability, relative to the other plans and current law. Milliman predicted
premiums would rise by $33.9 billion, over 10 years, under the AAF proposal (if
behavioral assumptions proved true) which would provide beneficiaries with
overall net savings of $7.4 billion.
Conclusion
In the 16
years since Congress created the Medicare Part D program, the prescription drug
market, insurance structure, and pricing practices have changed. Patterns
have emerged that make it clear the current system is encouraging undesirable behaviors that increase costs
for the government and consumers. Reforming the benefit structure in a way that
realigns the financial incentives of both the insurers and drug manufacturers
may help to reverse these trends by putting downward pressure on drug prices.
Such a substantial reform, however, requires careful consideration of the many
trade-offs that will result from those changes. Putting too much pressure on
drug prices could instead result in reduced innovation, fewer new treatments,
and restricted access to medicines.
Appendix
Assumptions
and Methodology
In the
estimates for total rebates collected, it is assumed that the average cost per
beneficiary using a given drug will increase 6 percent from 2017 to 2022.
Utilization of each drug is assumed to increase 16 percent, equal to the
expected increase in program enrollment during that time, according to the
latest Medicare Trustees Report. The deductible under
all proposals is assumed to be $485, as the Trustees estimate for 2022. In the
current law estimate, the initial coverage limit is assumed to be $4,490 (also
from the Trustees Report). For all other proposals, the initial coverage limit
(also the catastrophic limit) was calculated based on the plan’s OOP cap. For
these estimates, it is assumed that beneficiaries only take drugs for which a
manufacturer would be required to pay a rebate. These estimates also assume no
behavioral changes.
Further,
only drugs for which estimated average annual per beneficiary spending exceeds
the threshold at which a rebate would be required is included in the estimate
of total rebates that must be paid; thus, these estimates represent the low-end
of the amount likely to be collected. That said, the estimates for rebate
collections under current law and Pelosi’s plan are likely much closer to the
total collection amount than the estimates for the AAF and Finance proposals.
This is because the rebate collections begin at a lower spending threshold and
thus more of the total program spending is captured.
Limitations
It is
important to note that these estimates do not account for any new drugs that
have come to market or are expected to come to market after 2017. Further, these
estimates do not include rebates that will be required from all other drugs
provided after a beneficiary surpasses the threshold for which rebates are
required but have an average annual per beneficiary cost that is less than the
rebate threshold. Conversely, these estimates do not exclude drugs that may be
generic products.
[i] Current law does not require manufacturers to
pay Coverage Gap discounts for low-income subsidy (LIS) beneficiaries.
Disclaimer
https://www.americanactionforum.org/insight/competing-proposals-to-reform-medicare-part-d/#ixzz60RhyAU1Y
Follow @AAF on Twitter
https://www.americanactionforum.org/insight/competing-proposals-to-reform-medicare-part-d/#ixzz60RhyAU1Y
Follow @AAF on Twitter
No comments:
Post a Comment