Tara O'Neill Hayes, Josee Farmer April 2, 2020
Executive Summary
·
Diabetes cost the United
States $327 billion in 2017, becoming the most expensive chronic disease in the
nation.
·
Insulin costs, before
accounting for any rebates or discounts, comprise an estimated $48 billion (20
percent) of the direct costs of treating diabetes; after rebates, insulin
accounts for 6.3 percent of costs.
·
The average list price
of insulin increased 11 percent annually from 2001 to 2018, with average annual
per capita insulin costs now nearing $6,000. Because patients’
out-of-pocket costs are typically based on list price, their expenses have
risen substantially despite the decrease in net price for many of the most
commonly used insulin products over the past several years.
·
If the trends of the
past decade continue, gross insulin costs in the United States could reach
$121.2 billion in total spending (or $12,446 per insulin patient) by 2024, but
if more recent trends of much slower price growth prevail, insulin spending
could total $60.7 billion in 2024 (or $6,263 per patient).
The Rising Cost of Diabetes
Diabetes is now the most expensive chronic
condition in the United States.[1] One in every four U.S. health care
dollars is spent on someone with diabetes, and one in seven dollars is spent
directly on diabetes-related expenses.[2] The
economic cost of diabetes in the United States totaled $327 billion in 2017,
including $237 billion for direct medical costs and $90 billion in lost
productivity.[3] The 2017 total represents an average
annual increase of 6 percent from the 2012 estimated cost of $245 billion.[4]
The rising costs of diabetes largely tracks the
dramatic increase in the cost of prescription
insulin—which an estimated 8.3 million individuals use to control
their condition. Between 2012 and 2018, the price of available insulin
increased 14 percent annually, on average, and in 2016 insulin accounted for 31
percent of a Type 1 diabetic’s health care costs, up from 23 percent in 2012.[5] The rising cost of insulin has an
impact on both patients and society as a whole. One fourth of diabetic
patients, no longer able to afford their prescribed treatment plans, ration
their supply, which can be dangerous and potentially fatal.[6] And nearly three-fifths (57 percent)
of individuals with diagnosed diabetes are insured through a public program,
such as Medicare, Medicaid, or the Children’s Health Insurance Program (CHIP),
and these programs cover a disproportionate share (66 percent) of the costs of
diabetes.[7] In other words, taxpayers end up
footing most of the bill for diabetes treatments.
Given the rising costs, it is worth
understanding what is driving these increases. This analysis first details
increases in insulin prices and offers a projection for how much insulin will
cost in the coming years. It then examines what is driving these increases.
The Price of Insulin
Past Price Growth
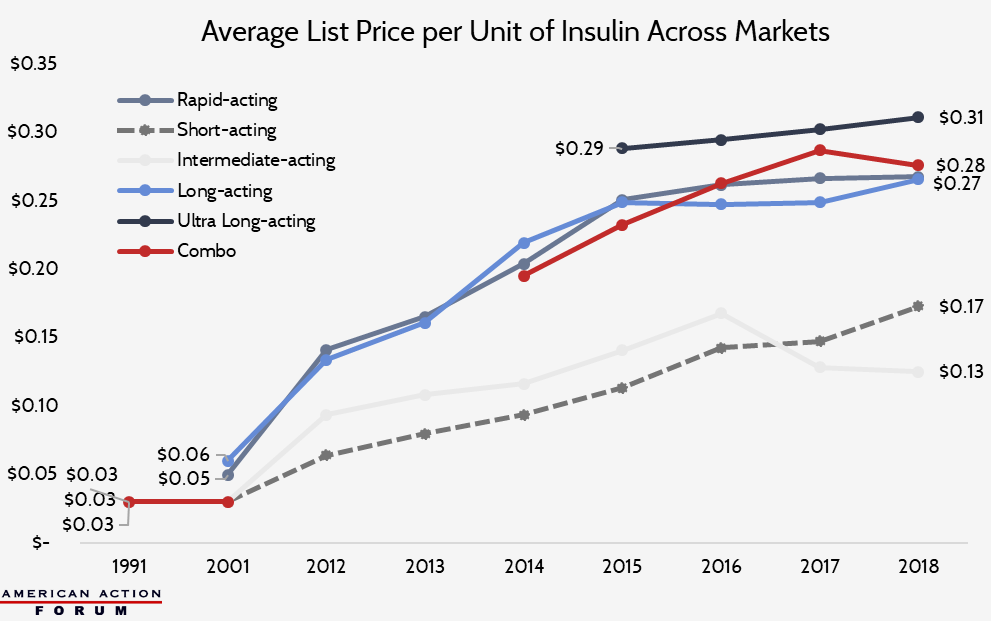
Since 1991, growth in insulin prices has been
accelerating, with a reprieve only in recent years. The list price of insulin
per milliliter in the United States increased, on average, 2.9 percent annually
from 1991-2001, 9.5 percent per year from 2002 and 2012, 20.7 percent annually
between 2012 and 2016, and 1.5 percent per year from 2016-2018.[8] .[9]
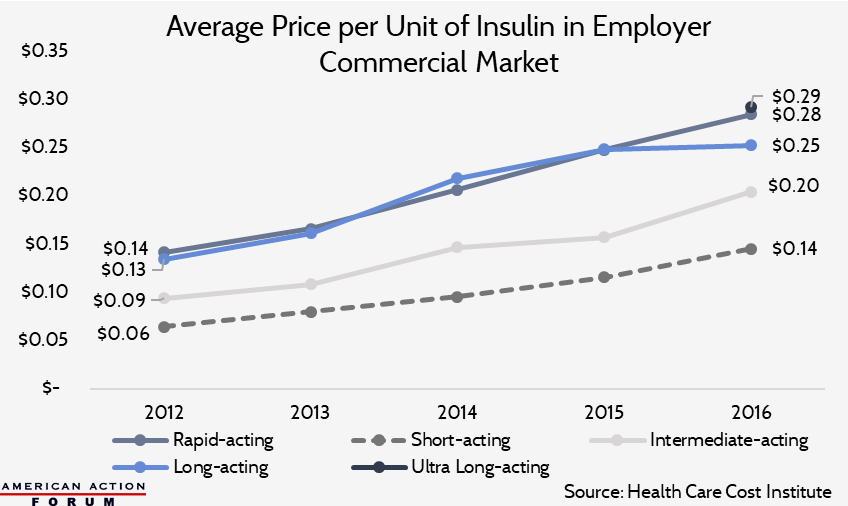
As the chart below shows, however, these
increases are driven not simply by price hikes for existing products, but by
higher prices for new products. Newer insulin products are more expensive than
older products. Since rapid-acting and long-/ultra-long-acting insulins are now
the most commonly used insulins, the rising cost of these medicines is
contributing significantly to rising average insulin costs per patient and
overall insulin spending.
The prices detailed above are list prices—and
the discrepancy between list prices and net prices due to rebates is likely
partially responsible for high insulin prices, as detailed below.
Insulin Spending in Medicaid
Examining Medicaid reimbursement for insulin
provides a useful window into market prices for insulin, as Medicaid, by law,
receives the “best price”
in the nation for all outpatient drugs. Medicaid reimbursements for insulin
have increased dramatically over the past decade. The chart below shows the
growth in the Medicaid reimbursement rate per milliliter (which typically
contains 100 units) of the various types of insulin. While the cost growth from
1991 to 2001 is noticeable, the increases from 2001 to 2014 were more rapid,
increasing an average of 9.1 percent annually primarily due to the introduction
of new insulin products.[10] These
price increases have resulted in Medicaid spending on insulin reaching $3.9
billion in 2018.[11]
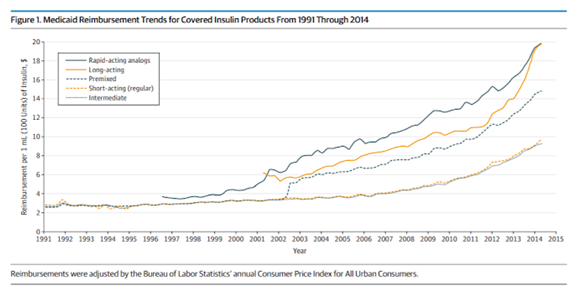
Source: American Medical Association [12]
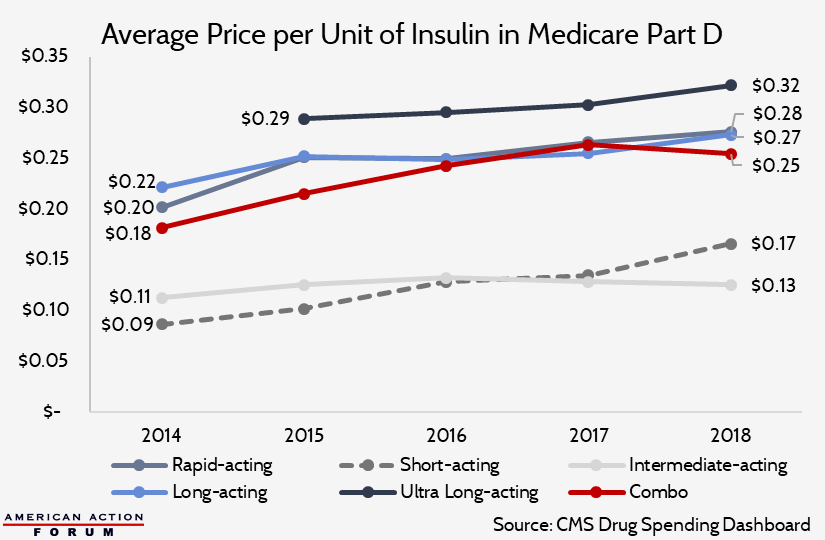
Insulin Spending in Medicare Part D
Medicare spending on insulin has also increased
exponentially over the past decade. Total Part D spending on insulin increased
10-fold from $1.4 billion in 2007 to $14.4 billion in 2018, more than 10 times
faster than enrollment.[13], [14] The top five insulin products in
2018 (in terms of use and total spending) accounted for $8.1 billion (56
percent) of all Part D insulin spending.[15] Spending per person increased 18
percent annually, from nearly $900 in 2007 to roughly $4,000 in 2016, and
beneficiaries’ average out-of-pocket (OOP) costs during this time increased 17
percent annually.[16]
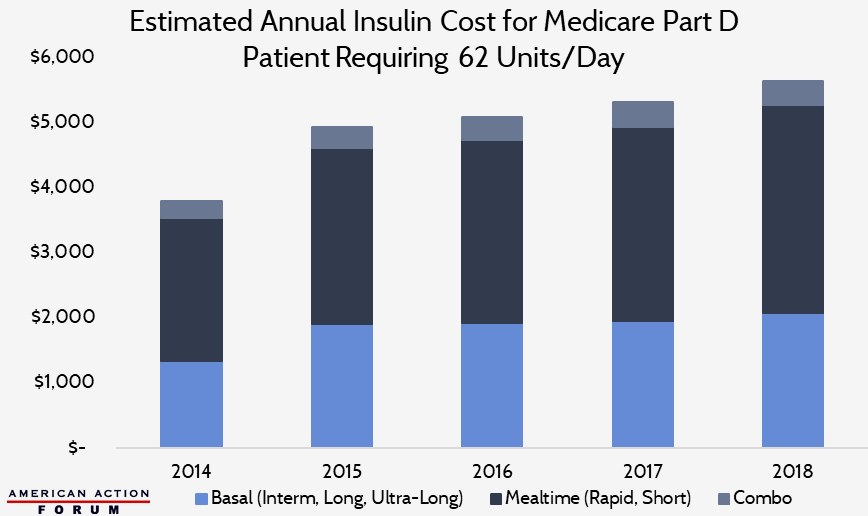
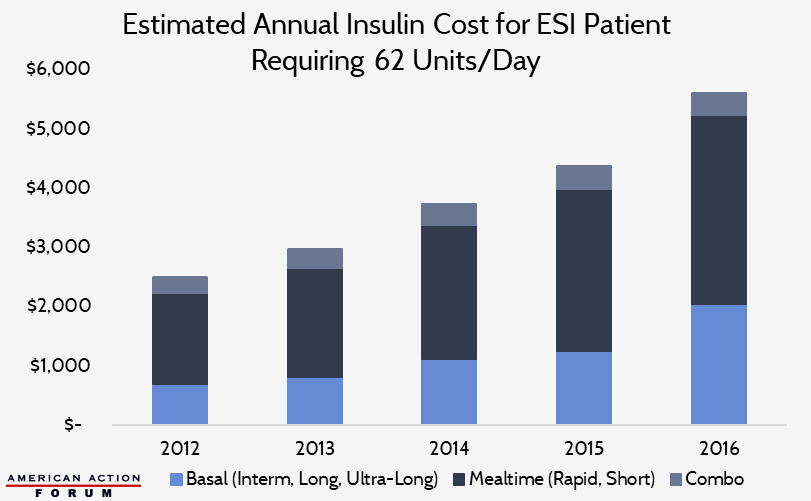
Typical Insulin Spending per Patient
According to the Health Care Cost Institute, the
average insulin user with employer-sponsored insurance (ESI) uses 62 units per
day (approximately 22 basal units, 36 mealtime units, and 4 units of
combination insulin).[17] The following chart shows the
estimated average annual insulin cost for a Medicare Part D patient taking a
similar dosage, based on pricing and spending data from the Centers for
Medicare and Medicaid Services’ Part D Drug Spending Dashboard.[18] Per capita insulin costs in
Medicare Part D, Medicaid, and ESI are all broadly similar and are estimated to
have surpassed $5,600 in 2018, as shown in the Appendix.
The Appendix further details spending and cost
information for Medicaid, Medicare Part D, and patients with ESI.
Estimating Future Costs
With more than 8 million Americans estimated to
be using insulin today at a cost of nearly $6,000 annually per person, insulin
costs (before rebates) account for roughly $48 billion (20 percent) of the
direct medical costs of diabetics.[19] If the share of diabetics requiring
insulin remains steady at 24 percent and 1.5 million Americans continue to be
diagnosed each year, gross insulin costs would increase more than $2 billion
annually if insulin prices and per capita utilization did not change. If
insulin list prices continued to increase at a rate similar to the trend
between 2012 and 2018, gross insulin costs in the United States could reach
$121.2 billion by 2024 (or $12,446 per insulin user), before subtracting
discounts and rebates. If prices continue to increase at the slower rate seen
between 2016 and 2018, gross insulin costs would increase to just $60.7 billion
in 2024 (or $6,263 per patient).
Why Are Prices Increasing?
A number of factors likely contribute to rising
insulin prices, but one of the largest is the existence of large rebates.
Rebates
The current practice of manufacturers offering
large rebates likely contributes to both increasing insulin prices and the limited
uptake of lower-priced products.[20] Pharmacy-benefit
managers (PBMs) are responsible for maintaining insurers’ drug
formularies, or list of prescriptions that are covered by a given insurance
plan, and they generate significant revenue through rebates on brand-name drugs
from manufacturers.[21] PBMs
incentivize drug manufacturers to offer competitively high rebates so their
specific products are included on formularies and given preferential placement.[22] Hence,
competition among drug manufacturers for top-tier allocation of their products
has driven ever-larger rebates, which naturally leads to higher list prices.[23]
While list prices are increasing significantly,
net prices (list prices minus rebates and other discounts) received by
manufacturers have increased much less drastically.[24] For example, Novo Nordisk reported
that between 2001 and 2016, the list price of the NovoLog vial increased 353
percent while the net price increased just 36 percent.[25] The
NovoLog FlexPen list price increased 270 percent between 2003 and 2016, while
its net price only increased 3 percent.[26] Eli
Lilly released similar information showing the list price of Humalog increased
27 percent from 2015 to 2019, while the net price decreased 14 percent.[27] Sanofi’s
latest pricing report shows that since 2012, the average list price for all its
insulin products increased 126 percent by 2018, while the average net price has
decreased 25 percent.[28]
Based on the data provided by these
manufacturers, as well as data from Pharmaceutical Care Management Association
(PCMA), insulin rebates average between 30 and 50 percent, and often reach as
high as 70 percent for the most commonly used insulin products, significantly
higher than the average rebate for other types of drugs.[29] For comparison, the Medicare
Trustees Report shows that rebates for all drugs averaged between 18 and 22
percent in Medicare Part D from 2015 to 2017, while rebates for all products in
Medicaid averaged 51 percent in 2016.[30], [31] Estimates of drug rebates in the
commercial market range from 12 percent to 30 percent in 2018.[32] PCMA maintains that its analysis of
rebates for insulin products indicates there is no correlation between list
price growth and the size of the rebate. It remains true, however, that insulin
rebates are larger, on average, than those provided for other types of drugs,
according to available data.
This discrepancy between list and net price has
a major impact on the amount that insurers and patients ultimately spend on
insulin. According to the American Diabetes Association’s (ADA) 2017 report on
the Economic Costs of Diabetes in the United States, after accounting for
discounts and rebates, insulin costs account for just 6.3 percent of overall
costs, ranging from 4.6 percent of costs for privately insured individuals and
7.2 percent of costs for those enrolled in public programs.[33]
Nevertheless, patients’ insulin costs, on
average, are increasing. Patients’ prescription out-of-pocket (OOP)
costs—increasingly calculated as a percentage of the cost (co-insurance),
rather than a fixed dollar amount (co-payment)—are typically based on a medicine’s
list price, rather than the net price. As list prices rise, so do patients’ OOP
costs. Further, the large rebates do not benefit insulin patients directly.
Insurers and PBMs use rebates primarily to reduce premiums for all enrollees,
rather than reduce patients’ OOP liability. Thus, diabetic patients generally
only benefit indirectly, through low premiums, from the significant rebates and
discounts offered for insulin products.
The rebate structure is also likely at least
partially responsible for the low utilization rates of the less expensive
insulin options currently on the market. Eli Lilly attempted to offer
lower-cost versions of both its pen and injection insulin products (Humalog
Lispro injections in May 2019 and Humalog Kwikpens in January 2020).[34] By
January 2020 (nine months after the release of the half-price Humalog
injections), only 14 percent of U.S. prescriptions for Humalog were for the
half-price version.[35] Pharmacists
and patients claim the half-price Humalog Lispro injections are not readily
available or that they are not covered by the patients’ insurance.[36] Novo
Nordisk announced it
would offer free, one-time insulin supply to patients in immediate need, as
well as expanded affordable options such as a $99 three-pack of vials or a $99
two-pack of their brand-name insulin pens. Last, Sanofi’s Insulin Valyou Savings
Program sets a fixed $99 monthly price on any combination of up
to 10 insulin vials/pens, but the program is only available to uninsured
patients.
If the cheaper products
are purchased (for which rebates are not provided), rather than the more expensive
products for which rebates are offered, insurers and PBMs may experience
reduced revenue. As a result, insurers and PBMs may be unlikely to encourage
patients to use the lower-cost options, perhaps by refusing coverage.
Competition Issues
Ninety-nine percent of
the insulin used in the United States is produced by one of three drug
manufacturers. The lack of robust competition allows insulin prices to remain
high, particularly for the uninsured and those with high cost-sharing insurance
plans. While the regulatory barriers hindering biosimilar insulin supply in the
United States recently expired, as explained here, it is unlikely that
new competition will enter the market overnight.
Regulatory Barriers
Finally, numerous legal
and regulatory changes affecting the broader health care market have likely
also impacted the price of medicines across the board. The Affordable Care Act
(ACA) included several provisions that either reduced drug manufacturer
revenues or increased the cost of selling drugs, primarily by expanding or
creating new programs for which drug manufacturers must provide significant
discounts. A previous American Action Forum study estimated that from
2012-2018, these policy changes cost the pharmaceutical industry roughly $140
billion.[37] Given that, it should not be surprising
that the price of medicines increased during this time.
Results of Increasing
Costs
Rising insulin prices
can cause severe consequences for diabetics. Roughly a quarter of American
diabetics reported rationing their insulin because they cannot afford the cost
of their full prescribed dosage.[38] In 2018, the ADA conducted the Insulin
Affordability Survey, and 39 percent of respondents indicated their insulin
costs had increased from the year prior, while 27 percent said that the increasing
costs of insulin had affected their insulin use or purchase in some way.[39] Of those who were affected, 26 percent
noted regularly taking less than prescribed, 23 percent noted having to change
to less expensive types or brands, and another 23 percent noted missing doses
weekly. Additionally, 36 percent said they were forced to make the choice
between insulin or other health-related services, 32 percent said they had to
make the choice between insulin or transportation, and 30 percent said they had
to make the choice between insulin or paying for their utilities.[40]
Conclusion
Diabetes is now the
costliest chronic condition in the United States, with one fourth of health
care expenditures in the United States spent on patients with diabetes. The
insulin costs for the estimated 8.3 million Americans who require prescription
insulin accounts for roughly 20 percent of the overall cost of treating
diabetes before rebates and discounts are factored in—although after rebates
are accounted for, insulin is responsible for 6.3 percent of overall costs. If
current trends continue, gross annual insulin costs could reach $121.2 billion
by 2024. While regulatory barriers hindering competition in the insulin market
are set to expire soon, changes to current drug pricing practices are likely
also needed to bring costs down.
Appendix
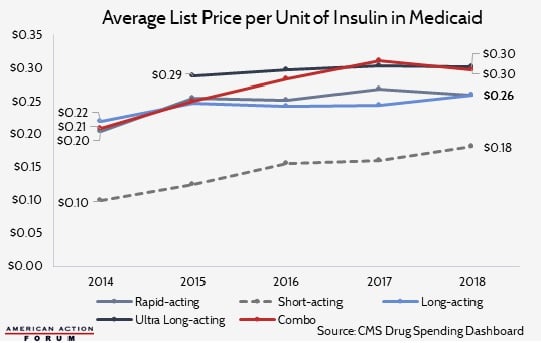
Insulin Costs in
Medicaid
From 1991 to 2014,
Medicaid reimbursements for insulin increased 17.1 percent annually from
roughly $42.8 million to $1.6 billion.[41] Between 2014 and 2018, spending
accelerated, averaging 24.2 percent per year for a cost of $3.9 billion in
2018. Though, as shown by the charts below, this increase was only partially a
result of price increases.[42] Much of the increased spending during this
period is due to rapid increases in Medicaid enrollment as a result of the
ACA Medicaid expansion.
The estimated average
cost per Medicaid patient using a standard dosage of insulin (22 units of basal
insulin, 36 units of mealtime insulin, and 4 units of combination insulin) is
depicted in the next chart, reaching $5,800 in 2018.[43]

Insulin Costs in the
Employer Market
According to the Health
Care Cost Institute, annual per capita insulin costs for diabetics with ESI
averaged $2,864 in 2012; by 2016, average costs had climbed to $5,705.[44] The chart below shows estimated annual
costs for an insulin patient in the ESI market, taking a standard dose of 62
units per day.[45]
Insulin Spending in
Medicare Part D
Total Part D spending on
insulin increased 10-fold from $1.4 billion in 2007 to $14.4 billion in 2018,
more than 10 times faster than enrollment.[46], [47] Another $367 million was spent on insulin
administration supplies (syringes, needles, pens, pumps, etc.) in 2018.[48] Spending per person increased 18 percent
annually from nearly $900 in 2007 to roughly $4,000 in 2016, and beneficiaries’
average OOP costs during this time increased 17 percent annually.[49] The average price per dosage unit
increased 10.1 percent per year from 2014 to 2018.[50]
Based on these data from
the Centers for Medicare and Medicaid Services’ Part D Drug Spending Dashboard,
the following chart shows the estimated average annual insulin cost for a
Medicare Part D patient requiring 62 units per day (22 basal units, 36 mealtime
units, and 4 units of combination insulin). Per capita insulin costs in Part D
surpassed $5,600 in 2018.
[1] https://connect.asmbs.org/07-2018/american-diabetes-association-report-diabetes-is-the-most-expensive-chronic-disease-in-america
[5] https://healthcostinstitute.org/diabetes-and-insulin/spending-on-individuals-with-type-1-diabetes-and-the-role-of-rapidly-increasing-insulin-prices
[7] https://care.diabetesjournals.org/content/diacare/suppl/2018/03/20/dci18-0007.DC1/DCi180007SupplementaryData.pdf
[8] http://www.natap.org/2019/HIV/ioi150073.pdf, https://www.uofmhealth.org/news/archive/201604/sugar-shock-insulin-costs-tripled-10-years-study-finds, https://healthcostinstitute.org/diabetes-and-insulin/price-of-insulin-prescription-doubled-between-2012-and-2016, https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Information-on-Prescription-Drugs
[9] https://healthcostinstitute.org/diabetes-and-insulin/spending-on-individuals-with-type-1-diabetes-and-the-role-of-rapidly-increasing-insulin-prices
[11] Authors’
calculation based on CMS Medicaid Drug Spending Dashboard data: https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Information-on-Prescription-Drugs/Medicaid
[14] 2018
estimates are authors’ calculations based on data obtained from CMS’s Medicare
Part D Drug Spending Dashboard: https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Information-on-Prescription-Drugs/MedicarePartD
[15] Products
include: Lantus Solostar, Levemir Flextouch, Lantus, Novolog Flexpen, and
Humalog Kwikpen U-100. Authors’ calculations based on data obtained from CMS’s
Medicare Part D Drug Spending Dashboard: https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Information-on-Prescription-Drugs/MedicarePartD
[17] https://healthcostinstitute.org/diabetes-and-insulin/spending-on-individuals-with-type-1-diabetes-and-the-role-of-rapidly-increasing-insulin-prices
[18] https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Information-on-Prescription-Drugs/MedicarePartD
[19] This
estimate does not account for the value of rebates provided for insulin as that
information is not publicly available and thus was not included in the study conducted
by the Health Care Cost Institute or the data available on the CMS Drug
Spending Dashboards which are the basis for this estimate.
[27]https://assets.ctfassets.net/srys4ukjcerm/4eLJOMYz0ZOsvxx8QqmxEb/111ae072aba877601c2e0cc836ded5dc/Lilly-2019-Integrated-Summary-Report.pdf
[28] https://www.sanofi.us/-/media/Project/One-Sanofi-Web/Websites/North-America/Sanofi-US/Home/corporateresponsibility/Prescription_Medicine_Pricing_2019.pdf?sf208075846=1
[30] https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/ReportsTrustFunds/Downloads/TR2019.pdf
[33] https://care.diabetesjournals.org/content/diacare/suppl/2018/03/20/dci18-0007.DC1/DCi180007SupplementaryData.pdf
[34]https://www.reuters.com/article/us-lilly-insulin/eli-lilly-to-launch-half-priced-versions-of-two-more-insulin-products-idUSKBN1ZD1JN
[35]https://assets.ctfassets.net/srys4ukjcerm/4eLJOMYz0ZOsvxx8QqmxEb/111ae072aba877601c2e0cc836ded5dc/Lilly-2019-Integrated-Summary-Report.pdf
[36]https://www.politico.com/newsletters/prescription-pulse/2019/10/11/access-issues-drug-shortages-dictate-pharmacy-fills-in-q3-780208
[37] https://www.americanactionforum.org/insight/understanding-the-policies-that-influence-the-cost-of-drugs/
[42] https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Information-on-Prescription-Drugs/Medicaid
[43] Utilization
rates have been increased from 40 units per day (used in the AMA study) to 60
units per day to better match today’s average utilization, as found in the HCCI
report: https://healthcostinstitute.org/diabetes-and-insulin/spending-on-individuals-with-type-1-diabetes-and-the-role-of-rapidly-increasing-insulin-prices
[44] https://healthcostinstitute.org/diabetes-and-insulin/spending-on-individuals-with-type-1-diabetes-and-the-role-of-rapidly-increasing-insulin-prices
[45] https://healthcostinstitute.org/diabetes-and-insulin/price-of-insulin-prescription-doubled-between-2012-and-2016
[47] 2018
estimates are authors’ calculations based on data obtained from CMS’s Medicare
Part D Drug Spending Dashboard: https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Information-on-Prescription-Drugs/MedicarePartD
[48] Authors’
calculations based on data obtained from CMS’s Medicare Part D Drug Spending
Dashboard: https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Information-on-Prescription-Drugs/MedicarePartD
[50] Authors’
calculations based on data obtained from CMS’s Medicare Part D Drug Spending
Dashboard: https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Information-on-Prescription-Drugs/MedicarePartD
https://www.americanactionforum.org/research/insulin-cost-and-pricing-trends/#ixzz6IYNwWIrA
Follow @AAF on Twitter
This comment has been removed by a blog administrator.
ReplyDelete