Christopher Holt July 20, 2018
It’s no secret that legislation and regulation
frequently cause unintended downstream challenges. For example—as detailed
in last week’s edition of the Weekly
Checkup—the creation of Medicaid “best price” unintentionally undermined drug
makers’ willingness to provide their medications at a discount for underinsured
(and uninsured) patients, leading to the creation of the now-bloated 340B Drug Discount Program. Even
well-intentioned and effective legislative efforts can cause problems for
policymakers down the road. Policies aimed at today’s challenges can evolve
into impediments to tomorrow’s innovation.
So it is with the myriad rules, regulations, and
statutes that have accrued over time to mitigate corruption within Medicare’s
fee-for-service payment system. In particular, the Stark Law has come under the
microscope recently, as policymakers look to further transition Medicare to
payment models that prioritize value rather than simply the number of
procedures. (The Stark Law also has implications for value-based payment
arrangements in the drug space as well—as detailed by AAF’s Tara O’Neill
Hayes here). Last week Centers for Medicare and
Medicaid Services Administrator Seema Verma singled out Stark as “one of the barriers
around value-based care.”
Simply put, the Stark Law seeks to prevent
physicians from referring patients to facilities or practices in which the
referring physician or a close family member has a financial stake. While this
prohibition made sense when it was passed, and the statute provides some safe
harbors to allow for exceptions, these restrictions have made some of the
innovative payment models currently being developed—as well as improved care
coordination—legally problematic.
More people than just Administrator Verma are
talking about the Stark Law. The House Ways and Means Committee held a hearing this week on “Modernizing Stark
Law to Ensure the Successful Transition from Volume to Value in the Medicare
Program,” in which Health and Human Services (HHS) Deputy Secretary Eric Hargan
testified in more detail about the obstacles Stark erects to improving the
Medicare program. And, in things you don’t see every day, former HHS
Secretaries Tommy Thompson and Kathleen Sebelius co-authored an op-ed further elaborating on the
impediment that Stark and other anti-kickback statutes are to innovation.
According to Administrator Verma, the Trump
Administration is aiming to “have something out by the end of the year.”
Perhaps, if the Thompson-Sebelius convergence is indicative, efforts to remove
barriers to innovative payment policies could provide a rare opportunity for
bipartisan cooperation on health care policy—and in an election year no less.
Chart Review
Tara O’Neill Hayes, Deputy Director of Health Care Policy
Tara O’Neill Hayes, Deputy Director of Health Care Policy
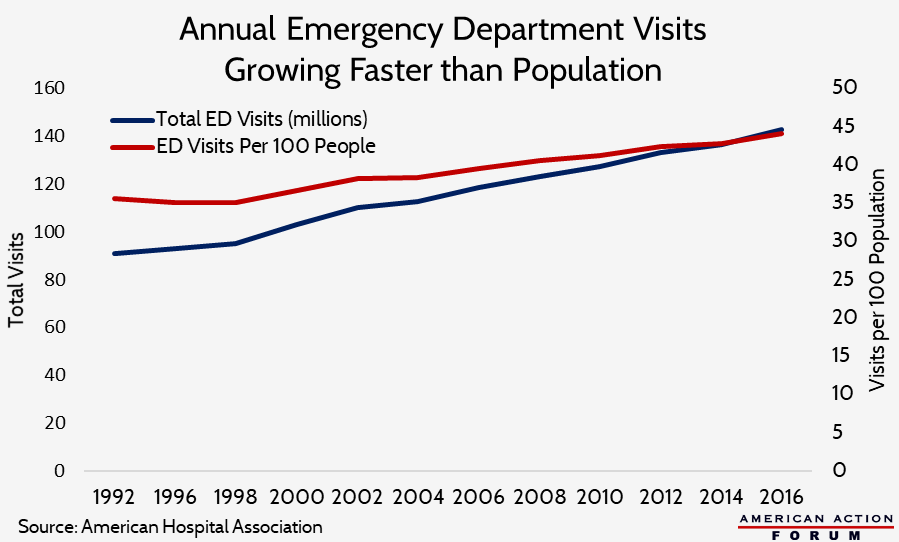
Americans’ use of emergency departments has been
rising steadily for decades, and rising at a rate faster than our population
growth, as shown in the chart below. This growth has occurred even as the
number of emergency departments has declined, putting even greater stress on
the remaining ones. As a result, hospitals struggle to use limited resources
efficiently and ensure those patients with true emergencies are treated in a
timely manner.
https://www.americanactionforum.org/weekly-checkup/clearing-obstacles-to-medicare-innovation/#ixzz5M5qwgrEG
Follow us: @AAF on Twitter
No comments:
Post a Comment