MaryBeth Musumeci
Follow @mmusumec on
Twitter and Robin Rudowitz Follow @RRudowitz on
Twitter
Published: Apr 30, 2019
Published: Apr 30, 2019
Like Idaho and Nebraska, Utah
voters supported a November 2018 ballot measure to adopt the full Medicaid
expansion as set out in the Affordable Care Act (ACA). Utah voters approved a full ACA expansion to
cover nearly all adults with income up to 138% of the federal poverty level
(FPL, $17,236/year for an individual in 2019), an April 1, 2019 implementation
date, and a state sales tax increase as the funding mechanism for the state’s
share of expansion costs. By implementing a full ACA expansion, Utah would
qualify for the substantially enhanced (93% in 2019 and 90% in 2020 and
thereafter) federal matching funds. The expansion population in Utah includes
childless adults ages 19-64 with income from 0 to 138% FPL and
parent/caretakers ages 19-64 with income from 60% to 138% FPL. The fiscal note from the ballot
initiative estimated that approximately 150,000 newly eligible
individuals would enroll in Medicaid in fiscal year 2020. However, Utah is one of 11 states (out
of the 21 states that allow state laws to be adopted via a ballot initiative)
that have no restrictions on how soon or with what majority state legislators
can repeal or amend voter initiated statutes.
The Utah legislature
significantly changed and limited the coverage expansion that was adopted by
the voters. Governor Herbert
signed Senate Bill 96 into
law on February 11, 2019. The state released an implementation toolkit that
follows the legislation in calling for multiple steps to implement an expansion
of Medicaid coverage to adults in ways that differ from a full ACA expansion
(Figure 1).
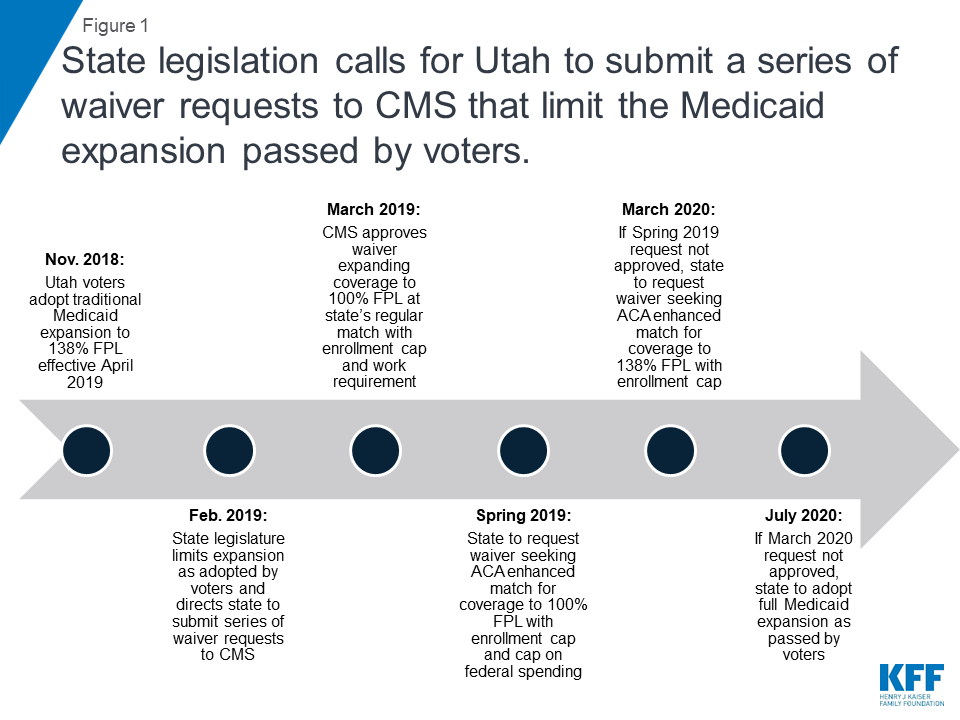
Figure 1: State legislation calls for
Utah to submit a series of waiver requests to CMS that limit the Medicaid
expansion passed by voters.
Utah’s Amended Waiver
On March 29, 2019, CMS approved
an amendment to Utah’s existing Section 1115 demonstration waiver to expand Medicaid to a
capped number of adults with income up to 100% FPL beginning on April 1, 2019
at the state’s regular Medicaid matching rate, not the enhanced ACA matching
rate.1 The
authority to cover this “Adult Expansion Population” expires on January 1,
2021. The Adult Expansion Population under the waiver includes childless adults
ages 19-64 with income from 0 to 100% FPL2 and
parent/caretakers ages 19-64 with income from 60% FPL to 100% FPL,3 a
more limited coverage expansion than the 138% FPL approved by the voters
(Figure 2). The state estimates that approximately 70,000 to 90,000 people will
be covered under the waiver with financial eligibility limited to 100% FPL,
about 40,000 fewer compared to a full ACA expansion to 138% FPL.4
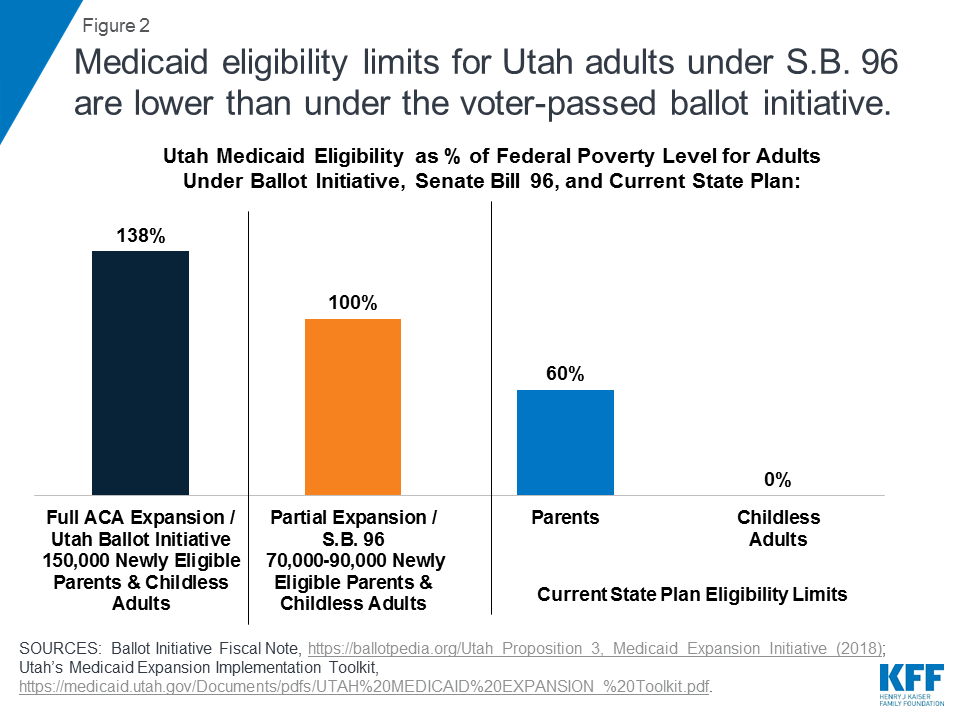
Figure 2: Medicaid eligibility limits
for Utah adults under S.B. 96 are lower than under the voter-passed ballot
initiative.
Instead of the 90% enhanced federal matching
rate tied to newly eligible adults under a full ACA expansion, Utah is
receiving its current, traditional federal matching rate of 68%, which will
result in higher state costs for expanding coverage to 100% FPL instead of a
full expansion to 138% FPL (Figure 3). Utah refers to the March 2019 waiver
amendment as the “Bridge Plan” because the state will seek further waiver
amendments as required by Senate Bill 96 and described in the text below.
Utah’s pre-ACA coverage expansion, authorized by its waiver prior to the Bridge
Plan amendment, is described in Box 1 below.
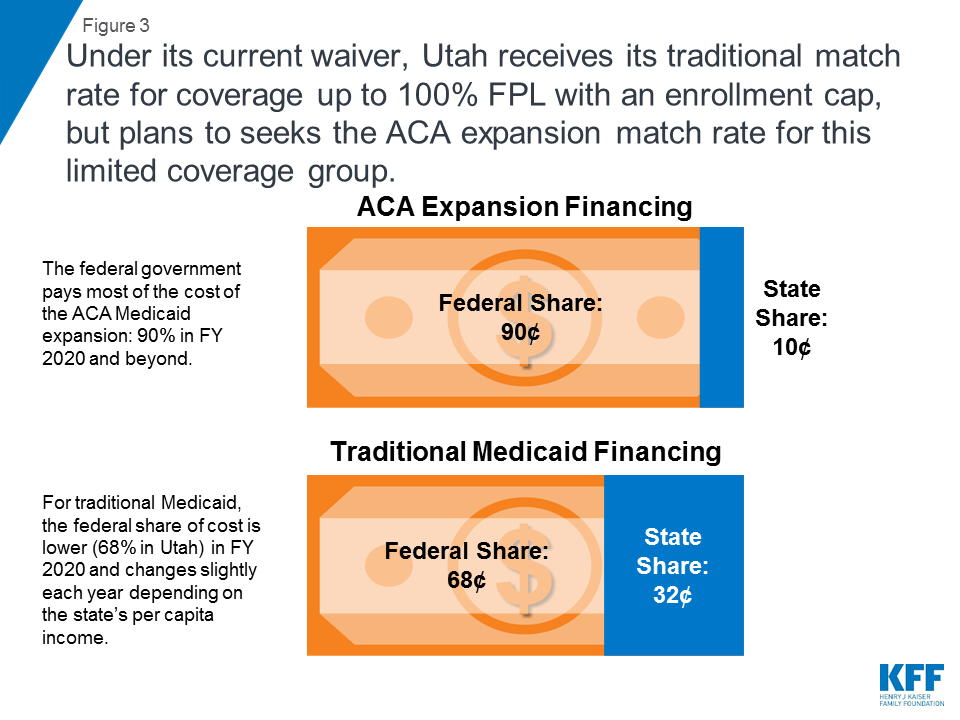
Figure 3: Under its current waiver,
Utah receives its traditional match rate for coverage up to 100% FPL with an
enrollment cap, but plans to seeks the ACA expansion match rate for this
limited coverage group.
Utah’s amended waiver includes
an enrollment cap to be imposed at state option on the Adult Expansion
Population, meaning that not all eligible people may be able to enroll in
coverage. The waiver allows the
state to close enrollment for the Adult Expansion Population, which could limit
enrollment further than the coverage estimates noted above. The waiver does not
specify a pre-determined maximum number of people to be covered but instead
allows the state to stop enrolling eligible people “if projected costs exceed
state appropriations.” If the enrollment cap is reached, the state will not
maintain a waiting list; instead, eligible individuals will have their applications
denied and will have to reapply for coverage when enrollment re-opens.
Consequently, individuals who apply at the beginning of a state fiscal year
could be more likely to gain coverage than those who apply later in the fiscal
year, even though they are otherwise eligible, if the state imposes the
enrollment cap. Individuals with lower incomes or higher needs, compared to
those already enrolled, might be barred from enrolling in coverage as a result
of the timing of their application due to the enrollment cap. No other state
currently has approval for an enrollment cap on adults who are eligible under
the ACA Medicaid expansion. As explained in Box 1, enrollment caps are no
longer necessary to ensure federal budget neutrality because the ACA now allows
states to access federal Medicaid funds for this coverage directly through the
creation of the new adult eligibility pathway and the availability of federal
matching funds.
Box 1: Coverage Expansion Under
Utah’s Waiver Prior to the ACA
In 2014, the ACA for
the first time authorized federal Medicaid matching funds for coverage for
nearly all nonelderly adults. Prior to 2014, federal Medicaid funds only could
be used to cover pregnant women, parent/caretakers, children, seniors, and
people with disabilities. Adults without dependent children were ineligible for
Medicaid, no matter how poor they were. Before the ACA, some states used
Section 1115 waivers to establish coverage expansions beyond the limits of
federal law. Because federal Medicaid funds could not be accessed directly to
cover these adults, these waivers included provisions to generate savings to
fund coverage expansions, such as limited benefit packages, premiums, and/or
mandatory managed care enrollment, and sometimes enrollment caps as a way to
limit federal spending and ensure federal budget neutrality.5 However,
budget neutrality is no longer a consideration for such coverage expansions
under waivers now that federal Medicaid law, as amended by the ACA, includes an
eligibility pathway and allows states to receive federal Medicaid matching
funds to cover nearly all nonelderly adults, including those without dependent
children, up to 138% FPL without the need for a waiver.
Utah’s existing
Section 1115 waiver was first approved in 2002, and included a pre-ACA coverage
expansion (called the Primary Care Network, PCN) to parents with income above
the state plan limit (60% FPL) and childless adults (for whom no state plan
coverage was available). As of March 2019, the PCN income limit was 100% FPL.
The PCN coverage expansion provided a limited benefit package of primary and
preventive services6 to
a capped number of these adults and was funded by reduced benefits for
traditional low-income (categorically and medically needy) parents. The March
2019 waiver amendment suspends authority for Utah’s pre-ACA PCN coverage
expansion and moves the 17,500 parents and childless adults in the PCN group as
of March 2019 to the new “Adult Expansion Population” (described in the text
above) effective April 1, 2019.7
Utah’s amended waiver also
includes a work requirement as a condition of eligibility for the Adult
Expansion Population, beginning no sooner than January 1, 2020.8 In
Utah, individuals subject to the work requirement must complete certain
activities within the first three months of each 12-month eligibility period or
qualify for an exemption. Those who fail to do so will lose coverage for the
rest of the year or until they fulfill the requirement. Required activities
include registering for work through the state’s online system, completing an
online employment training needs assessment, completing online job training
modules identified through the assessment, and applying for work with at least
48 potential employers.
What is Next?
Senate Bill 96 calls for Utah
to submit a subsequent Section 1115 waiver amendment proposal that includes a
request to receive the 90/10 ACA enhanced match for coverage up to 100% FPL
subject to an enrollment cap. This “Per Capita Cap Plan” is expected to be submitted to CMS in
the spring of 2019. The Per Capita Cap Plan would continue provisions in the
Bridge Plan (coverage up to 100% FPL, an enrollment cap, and a work
requirement), and add 12-month continuous eligibility, coverage lock-outs for
unspecified program violations, housing supports, elimination of hospital
presumptive eligibility, and a per capita cap on federal funds. The state
legislation does not explain how such a per capita cap would operate other than
to say that it would include an annual inflationary adjustment, account for
“differences in cost among categories of Medicaid expansion enrollees,” and
provide “greater flexibility to the state than the current Medicaid payment
model.”
If CMS does not approve the Per
Capita Cap Plan by January 1, 2020,9 the state will submit
another waiver amendment request seeking authority for a coverage expansion up
to 138% FPL with the ACA enhanced matching funds and an enrollment cap. This “Fallback Plan” also would include
coverage lockouts for unspecified program violations and elimination of
hospital presumptive eligibility. The Fallback Plan would continue the work
requirement but would not seek a per capita cap on federal funds.
If the Fallback Plan is not
approved by July 1, 2020, the state will adopt the full Medicaid expansion as
set out by the ACA and approved in the ballot initiative. This would include coverage of all eligible
adults up to 138% FPL at the ACA enhanced matching rate and would use a state
plan amendment instead of waiver authority. It would not include a work
requirement or enrollment cap as proposed in the waiver proposals described
above.10
Other states will be watching
for CMS’s response to Utah’s forthcoming waiver request seeking the ACA
enhanced federal matching rate for a partial capped expansion. The ACA provides enhanced federal matching
funds to states that expand Medicaid to nonelderly adults up to 138% FPL. To
date, CMS has allowed states to receive the ACA enhanced Medicaid matching
funds only if the entire expansion group is covered. Prior to Utah’s request,
Arkansas and Massachusetts sought waivers to receive the ACA enhanced match
while limiting coverage to individuals at 100% FPL, but CMS did not approve
those waiver requests. A separate brief explains
that relative to full expansion, a partial expansion with enhanced federal
matching funds could result in less coverage and higher federal costs. If
approved, Utah’s request for the ACA enhanced federal matching funds for a
capped, limited partial expansion will open a new chapter in the debate over
Medicaid in both expansion and non-expansion states.
No comments:
Post a Comment