Meredith Freed , Juliette Cubanski Follow @jcubanski on
Twitter , Anthony Damico , and Tricia Neuman Follow @tricia_neuman on
Twitter Published: Apr 20, 2022
While Medicare provides health and financial
protections to more than 64 million Americans ages
65 and older and younger adults with long-term disabilities, gaps in coverage
and high cost-sharing requirements can make health care difficult to afford,
particularly for people with modest incomes. Medicare beneficiaries are
responsible for Medicare’s premiums, deductibles, and other cost-sharing
requirements unless they have private supplemental coverage,
a Medicare Advantage plan that covers some of the cost-sharing, or have incomes
and assets low enough to qualify for the Medicare Savings Programs (which
provide assistance with Medicare Part A and Part B premiums and/or cost
sharing) and the Part D Low-Income Subsidy (LIS) (which helps with Medicare
Part D drug plan premiums and cost sharing). The Biden Administration has promoted awareness of
these programs for low-income beneficiaries in an effort to increase
enrollment.
To provide greater insight into the number and
characteristics of beneficiaries enrolled in these programs in the U.S. overall
and in each state, KFF created profiles of each state showing
enrollment of Medicare beneficiaries in the Medicare Savings Programs and the
Part D Low-Income Subsidy, and their demographic characteristics including
race/ethnicity, age, and gender. This data note provides an overview of these
programs and highlights findings from the state-level profiles.
TAKEAWAYS
·
In 2019, 10.3 million
Medicare beneficiaries, or 16% of all beneficiaries, were enrolled in the
Medicare Savings Programs. The share of state Medicare populations enrolled in
the Medicare Savings Programs varies from 7% in North Dakota to 33% in the
District of Columbia, due in part to differences across states in eligibility
criteria for these programs and poverty rates among the Medicare population.
·
Among the nine states
and the District of Columbia that have the highest share of Medicare
beneficiaries enrolled in the Medicare Savings Programs, eight either have
eliminated the asset test or have asset limits higher than the federal limit
(District of Columbia, Connecticut, Maine, Louisiana, Mississippi, Alabama,
Massachusetts, New York).
·
While Medicare
beneficiaries enrolled in the Medicare Savings Programs automatically qualify
to receive assistance through the Part D Low-Income Subsidy, the opposite is
not true, in part because the income threshold to qualify for the Part D
Low-Income Subsidy is higher. In 2019, nearly 1.6 million Medicare
beneficiaries were enrolled in the Part D Low-Income Subsidy but not receiving
premium or cost-sharing assistance through the Medicare Savings Programs,
including just over 1.1 million beneficiaries who were eligible but not
enrolled and nearly half a million (441,000) who did not meet eligibility
criteria.
·
Compared to Medicare
beneficiaries overall, the Medicare Savings Programs and Part D Low-Income
Subsidy disproportionately serve beneficiaries in communities of color,
beneficiaries under 65 with disabilities, and women, who tend to have lower incomes
and modest savings.
Overview of the
Medicare Savings Programs and the Part D Low-Income Subsidy
MEDICARE
SAVINGS PROGRAMS
Under the Medicare Savings Programs, state
Medicaid programs help pay for premium and/or cost-sharing assistance for
Medicare beneficiaries who have income and assets below specified levels, up to
135% FPL under federal guidelines ($18,347 for individuals and $24,719 for
couples annually in 2022) and limited assets (below $8,400 for individuals and
$12,600 for couples in 2022). Beneficiaries may receive help with Medicare’s
premiums ($2,041 in 2022 for Part B), deductibles ($1,156 for Part A, $233 for
Part B) and other cost-sharing requirements. Most low-income Medicare
beneficiaries who qualify for Medicare premium and cost-sharing assistance
also qualify for full Medicaid
benefits, which can include long-term services and supports and
other services such as dental and vision; these beneficiaries are referred to
as full-benefit Medicare-Medicaid beneficiaries.
In 2019, 12.3 Medicare beneficiaries were
enrolled in both Medicare and Medicaid. Of these beneficiaries, 9.1 million
received full Medicaid benefits, including 7 million who also received
financial assistance through the Medicare Savings Programs, and 2.1 million
with full Medicaid benefits who do not qualify for the
Medicare Savings Programs, though some states may choose to pay for Part B
premiums for these beneficiaries.
In total, 10.3 million beneficiaries received
financial assistance through the Medicare Savings Programs in 2019. This total
includes the aforementioned 7 million beneficiaries who also receive full
Medicaid benefits and 3.3 million beneficiaries who only receive premium and/or
cost sharing assistance (Figure 1).
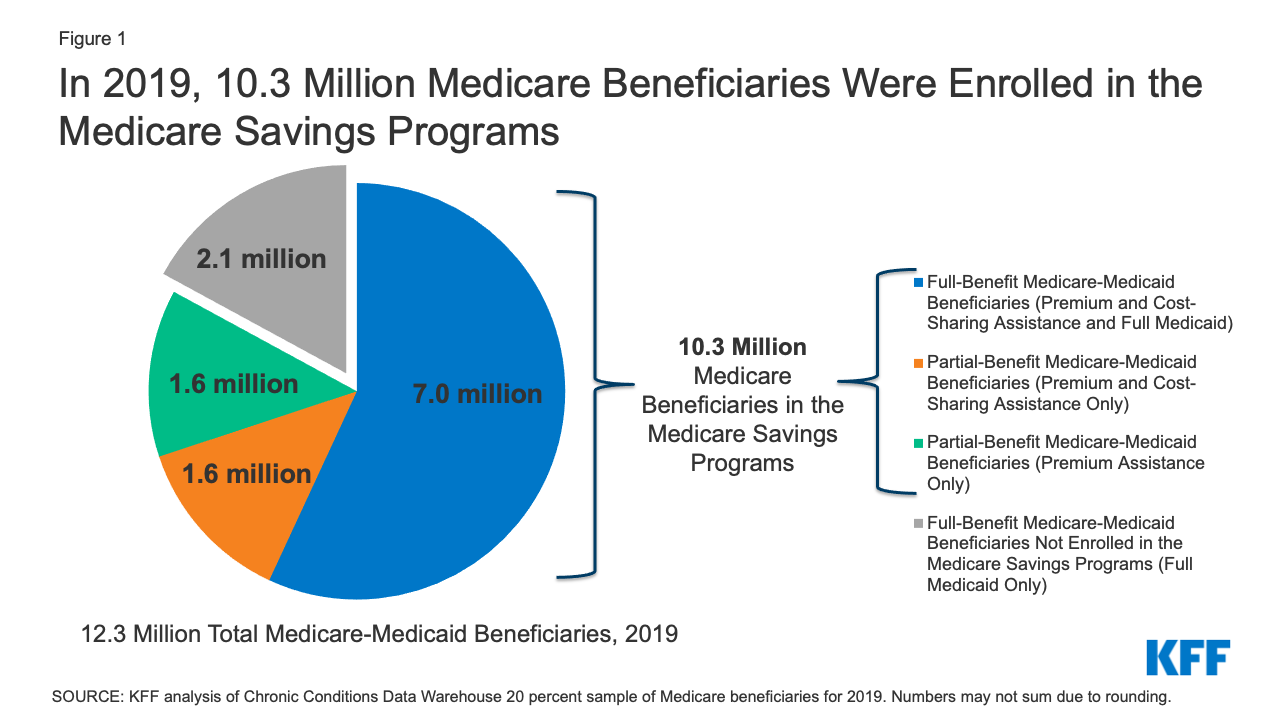
Figure 1: In 2019, 10.3 Million Medicare
Beneficiaries Were Enrolled in the Medicare Savings Programs
Low-income beneficiaries who receive only financial
assistance through the Medicare Savings Programs – meaning they qualify for
payment of Medicare Part A and/or B premiums and, in some cases, Part A and
Part B cost sharing but not full Medicaid benefits – are referred to as
partial-benefit Medicare-Medicaid beneficiaries. (See MedPAC MACPAC Data Book:
Beneficiaries Dually Eligible for Medicare and Medicaid — February 2022 for
a full discussion of the different types of Medicare Savings Programs.)
Of the 3.3 million Medicare beneficiaries who
received financial assistance through the Medicare Savings Programs, but not
full Medicaid benefits, half (about 1.6 million) received assistance with Part
B premium and cost-sharing assistance, while the other half received assistance
with Part B premiums but did not qualify for help with Medicare Part A and B
deductibles or cost-sharing requirements for covered services, despite having
incomes below 135% of poverty.
PART
D LOW-INCOME SUBSIDY
Under the Medicare Part D Low-Income Subsidy
(LIS), the federal government subsidizes premiums, deductibles, and cost
sharing for the Part D prescription drug benefit, providing varying levels of
assistance to beneficiaries at different income and asset levels up to 150% FPL
($20,385 for individuals and $27,465 for couples in 2022) and limited assets
(below $14,010 for individuals and $27,950 for couples in 2022). The 150% FPL
income threshold for LIS is higher than the 135% FPL threshold for the Medicare
Savings Program. Unlike the Medicare Savings Programs, the Part D Low-Income
Subsidy is a federal program and not part of the Medicaid program, nor is it
administered by the states, so states do not have the option of setting higher
income or asset thresholds for the Part D Low-Income Subsidy.
In 2019, 14.1 million (22% of all
beneficiaries) were enrolled in the Part D Low-Income Subsidy. The vast
majority (97%) of beneficiaries enrolled in the Part D Low-Income Subsidy
receive full LIS benefits, while only 3% receive partial LIS benefits.
Both full-benefit and partial-benefit
Medicare-Medicaid enrollees automatically receive full Medicare Part D LIS
benefits, meaning they pay no Part D premium or deductible and only modest
copayments for prescription drugs until they reach the catastrophic threshold,
when they face no cost sharing. Beneficiaries who receive partial LIS
benefits pay a reduced Part D premium and
deductible and 15% coinsurance for drugs until they reach the catastrophic
threshold, when they face modest copayments.
Individuals who do not automatically qualify
for LIS because they are not enrolled in the Medicare Savings Programs can
enroll if they meet income and asset requirements set by the federal
government. Depending on their income and assets, they could receive full
or partial LIS benefits. However, even if their income and assets meet Medicare
Savings Program requirements, individuals who qualify for Part D LIS are not
automatically enrolled in Medicare Savings Programs. While states are
statutorily required to initiate Medicare Savings Programs applications for
beneficiaries who apply for Part D LIS to help facilitate enrollment, CMS has noted that not all
states are meeting these standards.
|
Box 1: Medicare Savings Programs and Part D Low-Income Subsidy
Benefit Groups |
|
·
Full-Benefit Medicare-Medicaid: Full Medicaid benefits; Premium and
cost-sharing assistance through the Medicare Savings Programs; Full
Low-Income Subsidy ·
Full-Benefit Medicare-Medicaid Beneficiaries Not Enrolled in the
Medicare Savings Programs: Full Medicaid benefits only; Full Low-Income Subsidy ·
Partial-Benefit Medicare-Medicaid: Premium and cost-sharing assistance through
the Medicare Savings Programs; Full Low-Income Subsidy ·
Partial-Benefit Medicare-Medicaid: Premium Assistance only through the Medicare
Savings Programs; Full Low-Income Subsidy ·
Full Low-Income Subsidy: Part D premium and cost-sharing assistance; May be enrolled in
the Medicare Savings Programs depending on income and assets ·
Partial Low-Income Subsidy: Part D premium and cost-sharing assistance |
Findings
In 2019, 10.3 million Medicare
beneficiaries, or 16% of all beneficiaries, were enrolled in the Medicare
Savings Programs, but the share of state Medicare populations enrolled in the
Medicare Savings Programs varies by state, from 7% in North Dakota to 33% in
the District of Columbia (Figure 2).
States that have adopted more
generous income and asset thresholds – as well as states with higher poverty
rates among older adults – tend to have larger shares of beneficiaries enrolled
in the Medicare Savings Programs.
The federal government sets minimum income and
asset eligibility requirements for the Medicare Savings Programs, but states
can expand eligibility to beneficiaries with higher incomes and/or assets. As
of 2021:
·
Four states and the District of
Columbia have raised the qualifying federal poverty limits (Connecticut,
Indiana, Maine, and Massachusetts) above the federally defined minimum level.
For example, for the Qualified Medicare Beneficiary program where the income
limit is typically 100% of the federal poverty level ($12,880 for individuals
and $17,420 for couples in 2021), Indiana’s income limit is 150% ($19,320 for
individuals and $26,130 for couples), while Connecticut’s is 211% ($25,760 for
individuals and $34,840 for couples).
·
Ten states and the District of
Columbia have eliminated the asset test for the Medicare
Savings Programs, and three states have adopted an asset limit above the
federally defined minimum level (Figure 3).
These expanded income and asset limits only
apply to Medicare premium and cost-sharing assistance through the Medicare
Savings Programs. Beneficiaries still are required to meet state-defined
eligibility criteria to receive full Medicaid benefits, including nursing home
coverage and other long-term services and supports, in their state.
The variation across states in the share of
Medicare beneficiaries receiving premium and cost-sharing assistance through
the Medicare Savings Programs could be due to a number of reasons. One reason
might be the higher asset limits in some states: eight of the nine states and
the District of Columbia with the highest share of Medicare beneficiaries
enrolled in the Medicare Savings Programs either have eliminated the asset test
or have asset limits higher than the federal limit (District of Columbia,
Connecticut, Maine, Louisiana, Mississippi, Alabama, Massachusetts, New York).
This is not universally true, however; there are a few states with no asset
limit or higher asset limits, which have relatively lower shares of enrollment,
including Delaware, New Mexico, Oregon, and Minnesota.
Poverty rates among Medicare beneficiaries
also vary across states, although the relationship between poverty and Medicare
Savings Program enrollment rates is less clear. While some states with high
poverty rates (e.g., more than 25% of beneficiaries below 150% of poverty)
among the Medicare population have a relatively high share of beneficiaries
enrolled in the Medicare Savings Programs, (e.g., more than 20% enrolled:
District of Columbia, Louisiana, Mississippi, and Alabama), a handful of states
with high poverty rates have a relatively low share of beneficiaries enrolled
in the Medicare Savings Programs (e.g., West Virginia: 11%, New Mexico: 14%,
Georgia: 14%).
In addition to these factors, variations
across states in Medicare Savings Program enrollment may be related to
differences in the application process via state Medicaid agencies, which could
make it more difficult for beneficiaries in some states to apply, or
beneficiaries’ lack of awareness of the Medicare Savings Programs.
In 2019, nearly 1.6 million
Medicare beneficiaries (or 11%) received some help through the Part D
Low-Income Subsidy, but no premium and/or cost-sharing assistance from the
Medicare Savings Programs (Figure 4).
This includes more than 1.1 million people who
were not enrolled in the Medicare Savings Programs, even though they were
eligible, and another half a million beneficiaries (441,000) who did not
qualify for the Medicare Savings Programs because either their incomes and/or
assets were too high. These estimates do not include the approximately 2.1
million beneficiaries with full Medicaid benefits who do not qualify for the
Medicare Savings Programs but receive the Part D Low-Income Subsidy.
The share of beneficiaries who received
assistance through the Part D Low-Income Subsidy Program, but were not enrolled
in the Medicare Savings Programs, ranged from 1% in Connecticut to 21% in South
Carolina. Variations across states may be due to differences in the
administrative complexity of enrolling in the Medicare Savings Programs across
states (in contrast to the Low-Income Subsidy where beneficiaries apply through
the Social Security Administration), differences in methodologies in
how eligibility is determined for the Low-Income Subsidy versus the Medicare
Savings Programs in many states, and lack of awareness of the Medicare Savings
Programs, which may result in some beneficiaries applying for the Part D
Low-Income Subsidy but not the Medicare Savings Programs.
The Medicare Savings Programs
and Part D Low-Income Subsidy disproportionately serve beneficiaries in
communities of color, beneficiaries under 65 with disabilities, and women, who tend
to have lower incomes and modest
savings than beneficiaries who are White, 65 or older, or men
(Figure 5).
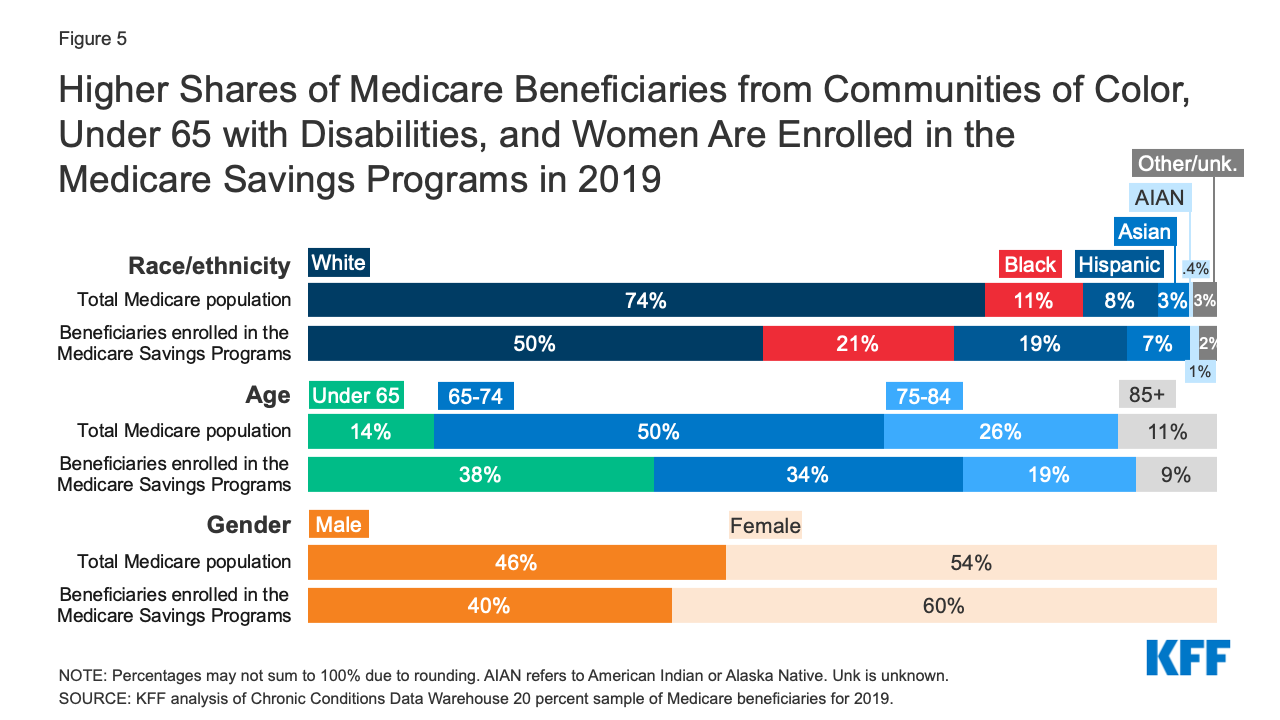
Figure 5: Higher Shares of Medicare Beneficiaries
from Communities of Color, Under 65 with Disabilities, and Women Are Enrolled
in the Medicare Savings Programs in 2019
Race/ethnicity. One in five (21%) of beneficiaries enrolled
in the Medicare Savings Programs are Black, nearly double the share of Black
beneficiaries (11%) in the total Medicare population. Similarly, 19% of
beneficiaries enrolled in the Medicare Savings Programs are Hispanic, more than
double the share of Hispanic beneficiaries (8%) in the total Medicare
population.
There are differences in the characteristics
of beneficiaries who are enrolled in these programs across states, which may be
due to state-level variation in the composition of the Medicare population, as
well as variation in the factors mentioned above, such as eligibility
thresholds and methods of determining eligibility, poverty rates, and the
characteristics of enrollees who have lower incomes. For example, in Alabama,
South Carolina, Maryland, and Georgia, Black beneficiaries comprise about a
quarter of each state’s Medicare population, but about half of Medicare Savings
Program enrollees in the state, ranging from 44% to 50%.
The share of Hispanic beneficiaries enrolled
in the Medicare Savings Programs also varies by state. In New Jersey, Colorado,
New York, and Nevada, Hispanic beneficiaries comprise one in ten of all
Medicare beneficiaries, but about a quarter of Medicare Savings Programs
enrollees in the state, ranging from 24% to 27%.
Age. The Medicare Savings Programs also reach a
disproportionate share of beneficiaries under age 65 who qualify for Medicare
due to long-term disabilities. For example, 38% of Medicare beneficiaries who
are under age 65 due to disability are enrolled in the Medicare Savings
Programs, nearly three times the share of under age-65 beneficiaries as their
share of the total Medicare population (14%).
The share of Medicare beneficiaries who are
under age 65 with long-term disabilities enrolled in the Medicare Savings
Programs also varies by state, ranging from 23% in California to 59% in New
Hampshire.
Gender. Women represent 60% of those beneficiaries
enrolled in the Medicare Savings Programs but 54% of the Medicare population
overall. There is somewhat less variation across states in enrollment by
gender, with the share of women enrolled in these programs varying from 52% in
Alaska to 63% in Alabama, Georgia, and Wyoming.
Overall enrollment patterns in the Part D-Low
Income Subsidy by race/ethnicity, age, and gender are
similar to the Medicare Savings Programs in large part due to the overlap of
enrollment in these programs.
Despite the important financial
protections the Medicare Savings Programs and Part D Low-Income Subsidy provide
to low-income people on Medicare, many low-income beneficiaries are not
receiving these benefits. Historically
these programs have had low participation, despite some state and federal efforts
to increase enrollment. Based on prior KFF work, the share
of Medicare beneficiaries with incomes below 150% FPL who are enrolled in the
Part D Low-Income Subsidy is estimated to be between 55% and 70%, while 50% to
65% are estimated to be enrolled in the Medicare Savings Programs (lower
because beneficiaries with incomes between 135%-150% FPL are not eligible for
these programs under federal guidelines) – though not everyone with incomes at
or below this level are eligible for either of these programs due to the asset
tests.
Additionally, certain groups of low-income
beneficiaries are less likely than others to be receiving assistance from the
Medicare Savings Programs, which could expose them to higher health care costs.
For example, based on our analysis of data from the Medicare Current
Beneficiary Survey, in 2019, nearly one in five Black and Hispanic Medicare
beneficiaries (19% and 17%, respectively) had incomes below 150% of poverty but
were not enrolled in the Medicare Savings Programs, compared to 11% of White
beneficiaries.
One reason for relatively low participation
rates overall in these programs could be the asset test used to determine
eligibility for both the Medicare Savings Programs and the Part D Low-Income
Subsidy, requiring beneficiaries to have countable resources, such as money in
savings and checking accounts, stocks, and bonds, below a certain limit. This
contrasts with eligibility requirements established under the Affordable Care
Act that use income, but not assets, to determine eligibility for Medicaid
expansion or Marketplace coverage. This means individuals living in states that expanded Medicaid up
to 138% FPL would be subject to an asset test when
they turn 65 or qualify for Medicare based on having a long-term disability in
order to get help from the Medicare Savings Programs with Medicare premiums and
cost sharing (unless they live in a state that has eliminated the asset test).
This “Medicare cliff” can result in low-income people losing access to valuable
financial protections that they qualified for prior to becoming eligible for
Medicare.
Discussion
In 2019, 10.3 million Medicare beneficiaries
received help through the Medicare Savings Programs. Enrollment in these
programs varies by state, due to differences in income and asset eligibility
criteria and administrative requirements across states. While 14.1 million
beneficiaries received help through the Part D Low-Income Subsidy, nearly 1.6
million of these beneficiaries did not receive premium or cost-sharing help
through the Medicare Savings Programs, because either they were ineligible or
did not enroll. Both programs disproportionately serve communities of color,
adults under 65 with disabilities, and women on Medicare, who tend to have
relatively low incomes and modest savings.
There has been some discussion among
policymakers of improving financial protections for low-income Medicare
beneficiaries, for example, by expanding income eligibility
thresholds for both the Medicare Savings Programs and Part D
Low-Income Subsidy, aligning eligibility criteria between these two programs,
and by raising or eliminating the federal asset test for the Medicare Savings
Programs, as some states have done. Such changes could provide stronger
financial protections to low-income beneficiaries living just above current
eligibility income and asset levels who are now responsible for payment of full
Medicare premiums, deductibles, and cost sharing. They would also increase
government spending, and do not appear to have strong prospects for passage in
the current political environment.
|
Methods |
|
This
analysis uses data from the Chronic Conditions Data Warehouse 20 percent
sample of Medicare beneficiaries for 2019. For this analysis, we use an
ever-enrolled approach for counting beneficiaries enrolled in the Medicare
Savings Program beneficiaries and the Part D Low-Income Subsidy, rather than
an average monthly measure, which may explain differences in our estimates
compared to other published estimates. This analysis excludes beneficiaries
living in Puerto Rico and the territories. |
This work was supported in part by AARP Public
Policy Institute (PPI). We value our funders. KFF maintains full editorial
control over all of its policy analysis, polling, and journalism activities.
Meredith Freed, Juliette Cubanski, and Tricia
Neuman are with KFF.
Anthony Damico is an independent consultant.
No comments:
Post a Comment