Reducing the impact of chronic diseases will require
payers and providers to get to the root causes of long-term illness, many of
which are attributable to the social determinants of health.
Healthcare providers
do their very best to understand everything they need to know about their
patients during the few scant minutes they are able to spend with each
individual.
Once or twice a year,
or maybe when a sore throat strikes, providers collect data on current
medications, chat about new problems, and order a prescription or two before
sending the individual on his way.
For many patients,
these self-contained interactions are perfectly adequate to address low-level
concerns or maintain good health.
But for many more,
especially those at elevated risk of developing chronic disease, episodic care
that begins and ends inside the clinic is simply insufficient to meet their
needs.
Chronic disease
doesn’t occur in isolation. Conditions such as diabetes, asthma, heart
disease, and obesity are all tied very closely to the environments, cultures,
and behaviors that surround individuals.
Food insecurity, lack
of housing or transportation, low educational attainment, the threat of
interpersonal violence, and social isolation create a complex web
of challenges that can contribute to deteriorating health, limited
functionality, and unnecessarily high spending.
As a whole, these
factors are known as the social determinants of health.
Defined by
the World Health Organization as “the conditions in which people are born,
grow, work, live, and age, and the wider set of forces and systems shaping the
conditions of daily life,” social determinants may be responsible for up to 90
percent of an individual’s long-term health and outcomes.
Commonly cited statistics pin the impact of purely
clinical care at between ten and twenty percent, while physical environments,
socioeconomic conditions, behaviors, and genetic predisposition account for the
vast majority of factors influencing outcomes.
As a result,
healthcare organizations are feeling the pressure to extend their reach beyond
the confines of the hospital campus and connect with patients where they live:
in their communities, at their work places, in their grocery stores, and at
their schools.
From sponsoring
community wellness programs to delivering targeted, clinically validated
patient education, healthcare providers are increasingly leveraging their
leadership positions to help local residents control their chronic diseases and
utilize healthcare resources more appropriately.
They are not
undertaking these efforts alone. As financial imperatives continue to
shift towards rewarding proactive approaches to care, payers are playing their
part in trimming costs and reducing the need for expensive acute services.
Both entities are
actively seeking out community-based partnerships and closer relationships with
public health officials, first responders, non-profits, social work agencies,
and other non-clinical organizations.
At the 2018 Value-Based
Care Summit hosted by Xtelligent Healthcare Media,
panelists and presenters shared insights and experiences about how to make this
multi-pronged approach to population health management work for some of the
most underserved populations in the country.
By combining the use
of data analytics to guide the allocation of scarce resources with some old-fashioned,
low-tech approaches to outreach and collaboration, healthcare providers and
payers are successfully combatting rising risks in vulnerable communities by
addressing the social determinants of health.
DEFINING
THE SCOPE AND SCALE OF SOCIOECONOMIC CHALLENGES
Every facet of an
individual’s life contributes towards his or her ability to successfully manage
health.
The luxury of taking
paid time off work for doctor’s appointments, affording child care, and hopping
in a working car to drive down to the clinic; the ability to understand and act
upon instructions from a clinician; the spare cash to pay for a prescription,
an MRI, or a follow up – all these factors depend on a person’s personal
behaviors, economic status, education, employment, family history, and cultural
expectations.
These challenges
impact rural populations just as much as inner city communities. In fact,
rural patients are more likely to face shortages of physicians,
a dearth of high-paying jobs with robust insurance benefits, and difficulties
accessing specialty care.
Non-metro communities
see higher rates of suicide, heart disease,
respiratory disease and stroke – and public health crises like the opioid
epidemic are hitting rural areas particularly hard.
At Atrium Health, a
large health system serving patients in North and South Carolina, providers see
just as many socioeconomic challenges in rural counties as in the urban areas
of the state, said Alisahah Cole, MD, Chief Community Impact Officer.
“When we map social
and economic factors like income levels and educational levels, and match that
data with the rates of chronic diseases, we can see that every county we serve
has at least one dark red area – a pocket of real vulnerability with huge
disparities,” she explained, showing a map of Atrium’s service area.
“People in urban
Mecklenburg are facing very similar issues to people in rural Cleveland County,
so that increases the complexity of the challenges we’re facing, as the
healthcare system, to address the social determinants leading to those
disparities.”
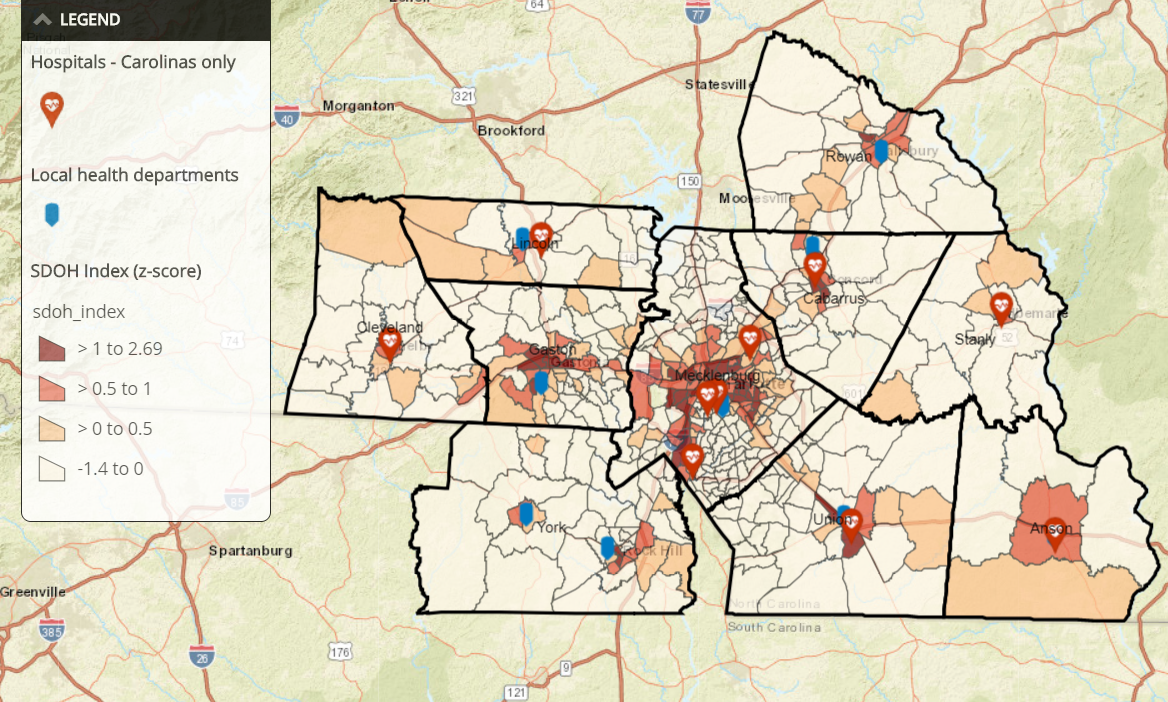
Socioeconomic disparities in North
Carolina communities
Source: Atrium Health
Healthcare systems
are using increasingly sophisticated data analytics strategies to identify the
specific challenges in each community, and to monitor the effectiveness of
interventions designed to get upstream of unplanned admissions and ED use.
Rising risk
individuals, or those on track to become high-spending, complex patients, are a
key focus for Atlanta’s Grady Health System, said Leslie Marshburn, Director of
Population Health.
“We know that
psychosocial needs are going to impact the speed at which someone hits the
markers of being a high-risk individual,” she said.
“As a safety net
hospital, we're really looking at those individuals who have the chronic
illnesses in conjunction with all the social, economic, behavioral, and
psychological factors that can contribute to poor health.”
“At Grady, we’re
using artificial intelligence to help us build out how we can identify patients
in the rising risk, moderate risk, and high risk categories. The challenge is
operationalizing that information and using those insights to allow the care
team to focus their resources appropriately.”
Hospital readmissions
are a popular place to start, she said, due to the potential return on
investment for avoiding admissions.
“We know that psychosocial needs are
going to impact the speed at which someone hits the markers of being a
high-risk individual”
“We look at everyone
who is at risk of an avoidable readmission within 90 days,” said
Marshburn. “Our tool looks at everyone who has touched our system in the
last 12 months or has an upcoming appointment in the next six months – that’s
around 160,000 people in any given time period.”
“That might seem like
a lot, but it does actually allow our care teams to get a handle on the scope
of the problem so they can prioritize and triage their outreach.”
Narrowing the field
to target interventions is essential, but it isn’t easy, added John Supra, VP
of Solutions and Services at the Care Coordination Institute in South
Carolina.
Understanding
patterns of utilization and getting ahead of costs is especially difficult in
communities where individuals may only access care in a life-threatening
emergency.
“We tend to have at
least marginally workable data on people who are traditional seekers of care,
and that can help with risk stratification and prediction. But what about
the people who aren’t in the system?” he asked.
About half of the
members of a given population do not seek care in a given year, he explained.
Yet at least some percentage will incur high costs in the near future when they
experience an exacerbation of chronic disease or another type of acute event.
“Where are these
people when they aren’t touching the healthcare system? Are they employed?
Do they have contact with faith-based organizations and schools? Are they
taking advantage of social services that we don’t know about?”
Marshburn agreed that
even the best population health analytics tools can’t be effective without any
data to use.
“We struggle a lot at
Grady with patients who aren’t represented in traditional data sets, especially
in data from payers,” she said.
“They’re
uninsured. They live in a cash world, and they don’t engage with the
financial system in ways that would create a consumer history. They might
have clinical records, but they’re often fragmented. They don’t have
regular sources of care that create the patterns we rely on for risk
stratification and case management, so we can’t track them in the way that we
would like.”
Most healthcare
organizations have not yet developed strategies to fill in those blanks and
reach the individuals who currently reside outside of the digital environment –
they still struggle to identify and care
for patients who have electronic health records.
“It’s difficult
enough to do any kind of analytics – I know that from experience. But the
people in the ether are the ones we need to get to, because the goal of
predictive analytics in the context of population health is to understand those
people before they end up in the ED or the hospital,” Supra stressed.
“And that will
require getting more insight into their communities and finding new connection
points to deliver education and preventive care.”
Hospitals, health
systems, and physicians are pillars of their communities, and quality
healthcare providers tend to enjoy a unique position of trust and influence
that can be invaluable for enacting change.
“The people in the ether are the
ones we need to get to, because the goal…is to understand those people before
they end up in the ED.”
In fact, few other
entities have such a powerful and wide-ranging impact on the very components of
health that may appear outside their direct control.
Healthcare systems
must take the lead when it comes to addressing fundamental challenges of
vulnerable communities, said Cole.
“We have found that
every community needs a convener,” she said. “As a healthcare system, a
lot of that burden is going to fall onto us. Atrium gives about $5
million a day in uncompensated care and other community benefits across our
region, and plenty of other health systems do comparable work. But we can't
do it alone. We can’t solve for all the problems, no matter how much we want
to.”
“What we can do is
pull everyone together and oversee the development of a cohesive, intentional
approach to addressing the social determinants of health. Someone has to
be responsible for coordinating those efforts, but we all need to be holding
each other accountable to really move the needle on population health.”
CREATING A
CULTURE OF CARE THAT BEGINS IN THE CLINIC
While advanced risk stratification and data analytics techniques
play an important role, many of their suggestions about how to address
socioeconomic disparities revolved around fundamental changes that don’t
require hiring a team of analysts or signing complicated vendor
contracts.
“We talk so much
about changing patient behaviors to improve chronic disease management and
educating them about how to work within the healthcare system, but we don’t
always focus enough on how we, as providers, need to change our attitudes
towards our patients,” asserted Caroline Morgan Berchuck, MD, Complex Care
Fellow at the Boston University Institute for Health Systems Innovation and
Policy.
“Value-based care
isn’t just a financial initiative. It requires culture change.
Being a good provider is about communication and working with patients on a
level that they understand. It’s about relationships, trust, and
respect.”
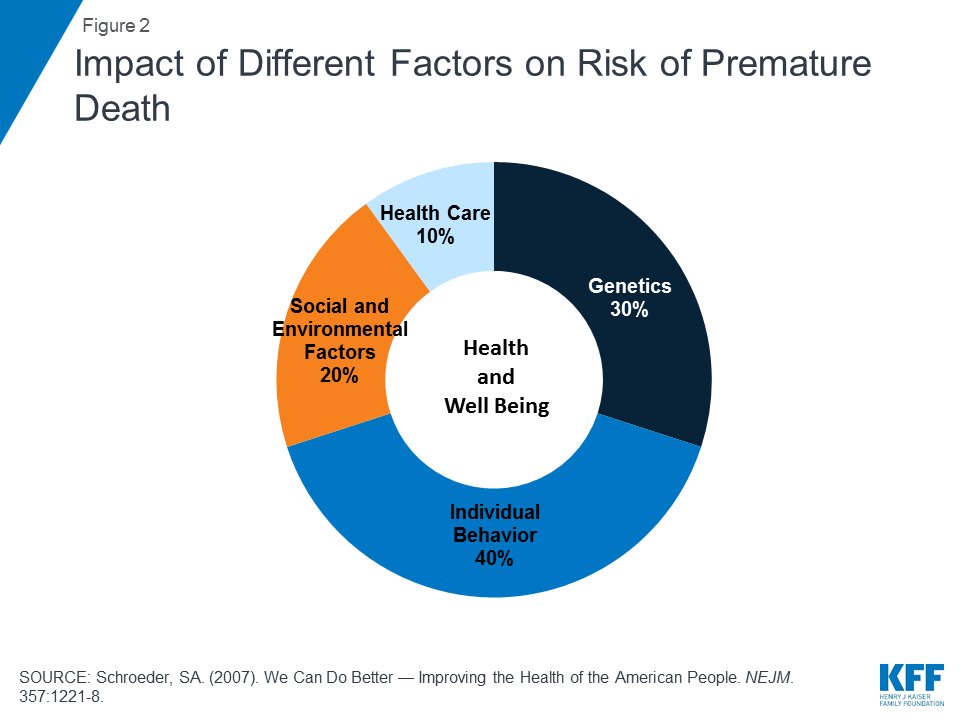
Source: Kaiser Family Foundation
The absence of trust
and respect from providers can have long-lasting impacts on how individuals
interact – or fail to interact – with the healthcare system, Berchuck
continued.
“I actually rotated
through Grady during medical school,” she said. “One of my first patients
as a medical student was in the A Tower at Grady – there are A, B, C, and D
towers.”
The patient, a
life-long Atlanta resident who was around 90 years old, told Berchuck that he
couldn’t believe he was being treated in the A Tower.
“Value-based care isn’t just a
financial initiative. It requires culture change.”
“When I asked why
not, he said that 60 years ago, the last time he needed the hospital, black
people weren’t allowed in the A Tower,” she recalled.
“His experiences at
that time had left him so averse to the healthcare system that he barely
interacted with it for sixty years. He had miraculously made it to 90 in
great health – but it just goes to show how some things that have nothing to do
with the clinical care he might have received can really affect personal decision-making.”
Offering a positive,
respectful patient experience is vital for success with value-based care,
especially when attempting to discuss sensitive SDOH topics such as economic
security, education, or interpersonal relationships.
“We need to be more
cognizant of those things, and we need to be more thoughtful and compassionate
with our patients,” urged Berchuck. “There is so much judgement around
diabetes, obesity, health literacy – even the inability to pay for certain
services. A lot of that comes from the clinicians themselves.”
“We need to be
careful that our patients don’t feel repulsed by their interactions with the
healthcare system if we’re going to truly support patients as they make
lifestyle changes and navigate their challenging circumstances. That
doesn’t cost a thing, but the ROI is huge.”
Extending
relationships outside of the traditional confines of the clinic and offering
services that meet patients where they are can be a powerful way to make
accessing care less daunting or uninviting, agreed Supra.
“The more we can do
locally, the better we’ll be at overcoming some of the cultural disconnect
between patients and providers,” he said. “We talk about hot spotting and
targeting interventions from a data perspective, but we can actually do that
from a physical standpoint, too, by bringing mobile clinics into areas that we
know are underserved or high-cost and rehabilitating empty storefronts or
grocery stores.”
“And when you staff
these clinics with people who are culturally competent, speak the same
languages, and have ties to the community themselves, you can create
connections that are very hard to replicate if you expect everyone to converge
on some centralized location away from where they live and work.
“The more we can do locally, the
better we’ll be at overcoming some of the cultural disconnect between patients
and providers.”
Going the extra mile
to create a welcoming, understanding, socioeconomically sensitive patient
environment has already paid off for Atrium Health, added Dr. Cole.
After using data
analytics to identify patients at high risk of readmission, Atrium looked
closer at socioeconomic factors that could contribute to those risks.
“We found that about
70 percent of our high-risk patients were food insecure,” Cole explained.
“Of that 70 percent, more than half were eligible for SNAP benefits but didn’t
realize that they qualified for assistance.”
In North Carolina,
the 13-page application for nutrition assistance is “extremely difficult” to
complete, she said. “I consider myself pretty well educated, and even I
struggled with it,” she admitted. “Talk about barriers to people
achieving good health, right?”
Atrium tasked one of
its community health workers with walking
applicants through the document to ensure they received the benefits they were
eligible for, she explained.
“On average, these
people received $200 a month in assistance,” Cole said. “Can you imagine
what a help that is to an elderly patient with diabetes, hypertension, and high
cholesterol living on a fixed income?”
Providers at Atrium
didn’t have to imagine the results. The impact was clear. The readmission
rate for the high-risk patients who received extra help with their applications
and subsequently utilized SNAP benefits plummeted by 67 percent.
“That doesn’t just
pack a punch financially – although the savings are certainly there. It also
positions the community health worker as a valuable resource and an ally, and
it makes sure that these individuals know Atrium is there to support
them. That’s an attitude shift within the community that goes beyond
dollars and cents.”
Atrium has also seen
success with its Community Resource Hub, an online
compendium of community services, such as housing options, legal aid,
transportation, and financial assistance for food, utilities, and education.
The website
catalogues services nationwide, and is freely available to the public as well
as to healthcare providers.
“This is the answer
to the question we get very often, which is ‘what do I do next when a patient
screens positive for a social need?’” said Cole.
“Now, a community
member can self-refer to services, or a member of our care team can do
it. And the service agency can talk back to us. It used to be that
I never knew what happened after I referred a patient to a community service
unless the patient came back and told me that she got what she needed.”
“With the hub, we now
have digital communication between these entities that enables us to take
action if we need to close that loop.”
LEVERAGING
PAYER POWER TO ENACT CHANGE IN THE COMMUNITY
Payers, too, are
offering more options for engagement, education, and access to care.
“Value-based care is
encouraging a lot more innovation on the payer side,” said Tina
Brown-Stevenson, Senior Vice President of Advanced Network Analytics at
UnitedHealthcare.
“One of the studies
we did with the United Health Foundation Board was around group prenatal visits. They have proven to
be unbelievably popular and successful, especially among low-income
women. They really enjoy and value the chance to meet other
mothers-to-be, share experiences, and spend some time in an environment that
supports them.”
“They have a group
session, step out for their individual exams with a nurse practitioner, then
come back together and have amazing experiences. That’s a lot more
attractive as an incentive to seek care than being told that they need to come
to the clinic for an appointment. They get their prenatal care, which is
good for everyone, and they get social interacts that they value on top of
it. It’s been so successful that we’ve been rolling it out all around the
country.”
At Humana, similar
community-based initiatives are designed to have net-positive impacts for all
parties involved, said Worthe Holt, MD, Vice President in the Office of the CMO
at Humana.
“This is the answer to the question
we get very often, which is ‘what do I do next when a patient screens positive
for a social need?’”
The social
determinants of health are a core component of the company’s Bold Goal program, which aims to
improve community health by 20 percent by the year 2020.
In San Antonio, one
of seven original communities serving as anchors for Bold Goal initiative,
diabetes is a major concern.
“The dinner table is
a central part of the Hispanic culture, where much of the diabetes challenge
lies,” Holt explained. “Sharing a meal while recounting the news of the
day, telling stories, and spending time with family is very important, but that
can make it difficult to make consistently healthy choices about what foods to
eat and how to engage in portion control.”
“Until you can help
people make better decisions about nutrition and diet without negatively
impacting a tradition that is so important to their social lives and family
structure, you aren’t going to make a real impact on the development of chronic
disease.”
Humana collaborated with grocery stores, the
YMCA, and food banks in the San Antonio area to deliver education, ensure food
security, and share resources related to managing diabetes effectively.

Results from the San Antonio Bold
Goal community
Source: Humana
“So instead of just
treating diabetes reactively, we worked with the community to offer more
advantageous placement of healthy food alternatives, cooking classes and other
education for individuals so they could add some new, lighter meals to their
repertoires without feeling like they are making some kind of unsustainable
lifestyle change,” said Holt.
By early 2018,
the results included a 5.1 percent
improvement on the CDC-validated Healthy Days measure for seniors living with
diabetes, as well as 5 percent increases in biannual hemoglobin A1C testing and
the use of diabetes statin therapies.
While health systems
like Grady and Atrium tend to view their coverage areas in terms of entire
geographic regions, payers like Humana and UnitedHealthcare are in the slightly
different position of being financially responsible for only a portion of
individuals in any given community.
Yet Bold Goal
projects are open to non-Humana members as well as the company’s health plan
beneficiaries, says Holt.
“The Bold Goal and
our other work around social determinants is really aligned with the ethos of
value-based care,” he said. “We’re going to work with underserved
populations, and we’re going to work with people experiencing socioeconomic
hardships. It’s going to improve the health of the community – and by the
way, it’ll benefit some Humana members, too.”
“Even the tools we’re
developing are intended to be payer agnostic. Most physicians work with
multiple payers, so it doesn’t make much sense to add to their existing burdens
by restricting tools and resources to just our members. If we can produce
tools and strategies that can bring value to the entire patient panel, then
Humana benefits as much as the physician and all those patients.”
FOSTERING
EFFECTIVE COLLABORATION IN A CHANGING FINANCIAL LANDSCAPE
An open mindset and a
non-traditional view of responsibility are vital for creating the transparency
and collaboration that will start to make a dent in the nation’s
socioeconomic disparities.
As value-based care
takes hold across more and more payer-provider relationships, both parties will
need to make adjustments to the way they view historical competitive
differentiators, such as data assets and the volume of patients served.
“If we can produce tools and strategies that can bring value
to the entire patient panel, then Humana benefits as much as the physician and
all those patients.”
“Collaboration is
truly the name of the game, and that will definitely include collaboration
between payers,” said Holt. “For our part, we are working with CMMI and CMS to
improve the data assets we can use to make valid inferences and conduct
meaningful analytics. We need more than just the population of one
payment model from one payer to get a true sense of the patterns and trends that impact
health.”
“Aggregated data is
essential. We’re talking to other payers at the CMO and CEO level to try to get
a group of individuals together who are willing to share de-identified
information and create more actionable insights for everyone.”
Payers have a unique
level of visibility into those patients who do leave a digital audit trail, but
they need clinical data from providers to maximize their analytics
capabilities, said Brown-Stevenson from UnitedHealthcare.
“Increasingly, we’re
getting data from providers who have electronic health records,” she
said. “And we’re working through some of the trust issues that surround
data sharing. But a lot of us are still stuck in the fee-for-service
mindset, where we have these parameters around who’s staying in our network,
who’s using our formulary, and who’s outside of our zone of caring, more or
less.”
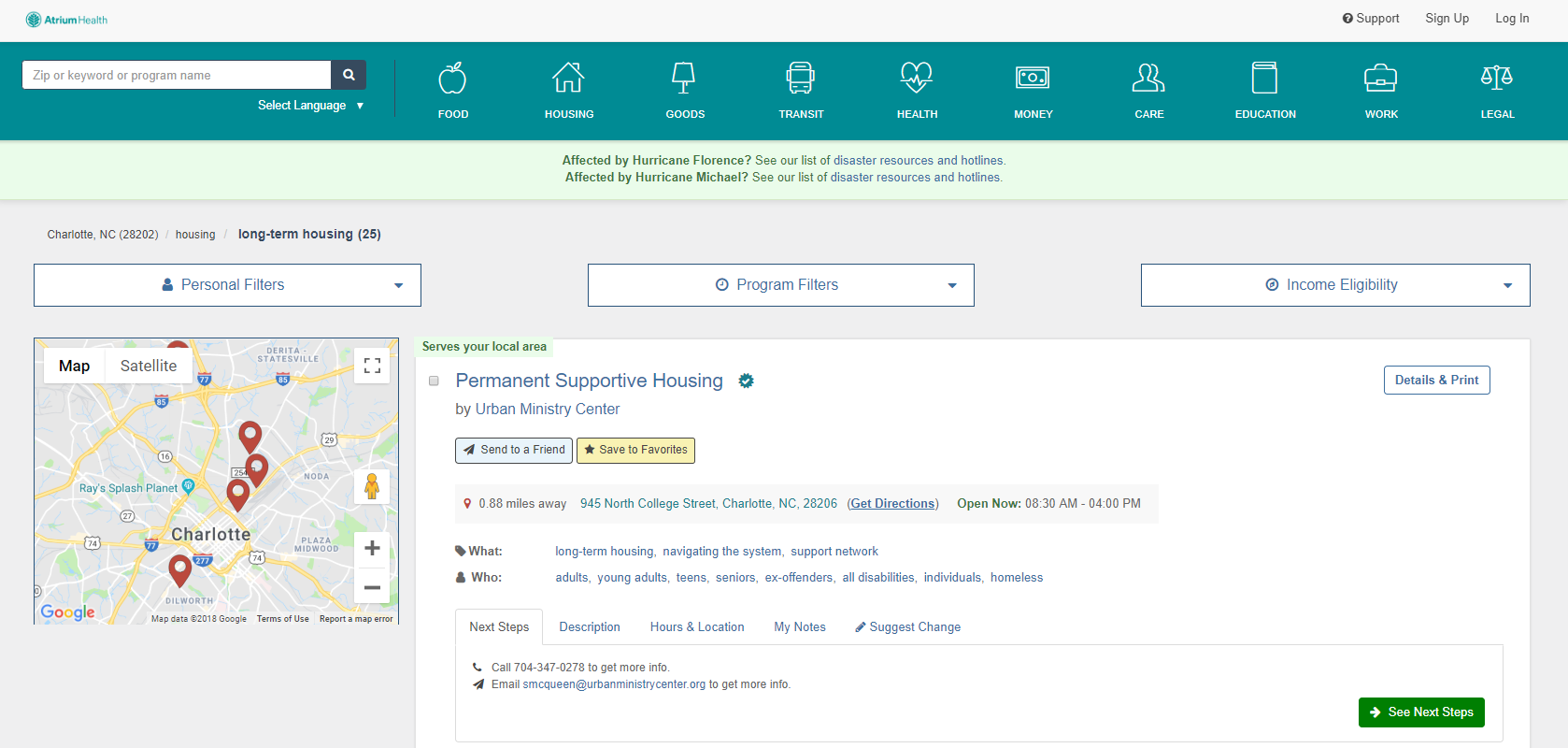
Community Resource Hub from Atrium
Health
Source: Atrium Health
“Those distinctions
aren’t going to help in the value-based care world,” said
Brown-Stevenson. “Integration of data will help. Delivering better
evidence-based care will help. Data is extremely important to our ability
to manage individuals, but we can’t do it all by ourselves. No one can.”
For providers,
getting access to the results of those analytics, as well as accessing care coordination data such
as admission, discharge, and transfer (ADT) notifications, will significantly
boost their ability to be proactive and reduce costs, says Berchuck.
“The integration of
the payers with the provider delivery system is really critical,” she
said. “In most primary care practices, you don’t have any way of finding
out if your patient is in the hospital. The hospital is on a different
EHR, or they didn’t call the PCP when they were supposed to – now you’re left
with a patient who has had 18 medication changes and a surgery, and you can’t
do the follow up that you would do if you knew about it.”
“Data is extremely important to our ability to manage individuals,
but we can’t do it all by ourselves. No one can.”
“Payers have such
broad visibility into the pharmacy, the hospital, the specialists, and pretty
much everything else that is happening to a patient. We need to keep
working on integrating that data more effectively into the clinical delivery
system.”
Creating alignment
between payers and providers will support the ongoing shifting of incentives
towards care that takes the social determinants of health into account.
Continuing to reward
healthcare providers for approaching healthcare in a person-centered, holistic
manner will produce exponential gains in financial and clinical outcomes.
“When the right
incentives are in place, we see that people are excited about this and looking
forward to engaging,” said Holt.
“We see consumers recognizing that they are
getting a more satisfactory experience, and we’re pleased to see that they are
pushing for even more change. Employers clearly are, as well. As we
demonstrate that value-based care improves quality and reduces expenses across
the board, it’s going to have a snowball effect.”
“It’s not going to
happen tomorrow, but I am convinced it will happen much more quickly than we
might have thought just a few years ago. We’re making excellent progress,
and it isn’t going to slow down any time soon.”
The results of
investing in communities and addressing social determinants can manifest in a
variety of ways, said Dr. Cole, and can truly change lives for the better.
“I'm a kid from one
of those dark red areas,” she said. “Statistically, I should not be standing up
here on this stage today. There are people like you who invested in me, so
never underestimate the power you have as an individual to impact someone's
life.”
“If we all committed
to work on social health and wellness together, just think about how much more
of an impact we can have. We want our communities to be better for us
being there. That’s our vision at Atrium Health: that the communities we
serve are the first and best choices to live in.”
This article was originally published on October 31, 2018.
https://healthitanalytics.com/features/combating-chronic-disease-through-the-social-determinants-of-health
No comments:
Post a Comment