Tara O'Neill Hayes June 11, 2019
Executive
Summary
·
Congress is considering reforms to the Medicare Part D program
that include moving the current Coverage Gap Discount Program (CGDP) to the
catastrophic phase of coverage.
·
Under current law, the maximum rebate amount required of
manufacturers for a given drug in 2020 is $3,698, regardless of the drug’s
cost, and the majority of mandatory rebates are paid for drugs that cost
$480-$580.
·
If manufacturers were instead required to pay a rebate in the
catastrophic phase, a much greater share of the rebates paid would be for the
most expensive drugs.
·
This reform would result in the mandatory rebate amount increasing
with the drug’s price, which would provide an incentive against price
inflation—an incentive the current system lacks.
Introduction
In the 16
years since Congress created the Medicare Part D program, the prescription drug
market, insurance structure, and pricing practices have changed. Patterns
have emerged that make it clear the current system is encouraging undesirable behaviors that increase costs
for the government and consumers. Reforming the benefit structure in a way that
realigns the financial incentives of both the insurers and drug manufacturers
may help to reverse these trends by putting downward pressure on drug prices.
There are
currently four phases of coverage: a first, where the beneficiary covers all
costs up to the deductible; a second, the initial coverage phase; a third (the
“coverage gap”), when the manufacturer now covers 70 percent of costs; and a
fourth, the catastrophic phase, when the government covers 80 percent of costs
and the insurer 15 percent. The beneficiary is responsible for some costs in
all four phases.
Congress
is considering providing beneficiaries with
an out-of-pocket (OOP) cap and reducing the government’s share of the costs in
the catastrophic phase while increasing insurer’s liability. These changes are
a good start, but alone they are insufficient to provide significant relief for
beneficiaries or put meaningful downward pressure on drug prices. Prior work by
the American Action Forum details why this is so and proposes a more
comprehensive reform of the benefit structure, including moving the mandatory
drug manufacturer rebates from the coverage gap to the catastrophic phase, as
shown below.

This
paper provides new analysis of the potential impacts of such a reform. It looks
at the rebates that would result from requiring rebates at various rates from
drugs at different prices.
The
Proposed Reform
The
current CGDP limits the mandatory rebate amount because the coverage gap only
covers a limited amount of expenditures. In 2020, the most that a drug
manufacturer will be required to pay in coverage gap rebates for a single drug,
now that the mandatory rebate is 70 percent, is $3,698.[1] Any
drug costing $9,303 or more will require a payment of this amount and no more.
Accordingly, the existing structure does not provide any incentive to drug
manufacturers to limit prices once they’ve exceeded the catastrophic threshold.
By requiring the discount instead to be paid in the catastrophic phase, which
has no limit other than the end of the year, the mandatory rebate will increase
with the price of the drug. This change should—at least more than the current
system—discourage price growth.
Further,
this change will target the rebate toward costlier drugs. MedPAC found that
under the current CGDP, diabetic therapies are responsible for 31 percent of
rebates paid; asthma and chronic obstructive pulmonary disease (COPD) drugs are
responsible for 12 percent, and 11 percent are paid for anti-coagulants.[2] The
average price of these medicines is $480-$580 per claim.[3] Alternatively,
if the rebates were collected in the catastrophic phase, MedPAC estimates that
antineoplastics (chemotherapy) would account for 20 percent of the rebates;
antivirals would be responsible for 15 percent; diabetic therapies, 11 percent;
analgesics and anti-inflammatory drugs would account for 9 percent; central
nervous system agents another 9 percent; and Multiple Sclerosis drugs would
account for 8 percent.[4] The
price of these drugs ranges from a few thousand to more than $30,000.[5]
If the
OOP limit (which would trigger a move into the catastrophic phase) was set at
$2,500, the total amount of drug expenditures that would be incurred by all
parties at that point would equal $8,695 in 2020. For comparison, under current
law, beneficiaries themselves are expected to spend $2,652 OOP before reaching
catastrophic coverage in 2020—with a True OOP (TrOOP) of $6,350—and total drug
expenditures will equal $9,303, if the beneficiary is only taking brand-name
drugs.[6]
Understanding
Different Rebate Rates
According
to analysis by actuarial accounting firm Milliman, 9 percent was estimated to
be the rebate discount rate in the catastrophic phase at which overall
manufacturer rebates would be roughly equal to what they are expected to be
under current law.[7]
This
figure provides a useful starting point for analyzing various discount rates.
If the manufacturer rebate were moved to the catastrophic phase and set at a
rate of 9 percent with a catastrophic threshold limit of $2,500, the break-even
price, at which point the rebate would be equal to the amount currently
required in 2020, is $49,784. Every manufacturer with a drug costing more than
this will pay more under these parameters than under the current system.
Further, every manufacturer with a drug costing more than $8,695 will pay
something, though it will be less than what they pay now if the cost is below
that break-even price. (Technically, all drugs provided to beneficiaries after
they’ve reached the catastrophic phase will require the payment of a rebate,
regardless of price, but it is impossible to know what those drugs might be, if
their cost is less than $8,695, and it may simply be poor timing that they
become subject to the rebate requirement.)
Of
course, even if overall rebates are the same, some manufacturers would fare
better and some would fare worse, depending on the prices of their drugs and
their utilization rates. Considering prices, rather than annualized costs, is
relevant here because there are many drugs for which a single dispense will
push beneficiaries into the catastrophic phase. In 2017, there were 152 drugs
for which a single claim exceeded the catastrophic threshold. There were nearly
2 million claims for these drugs, resulting in total spending of $24.6 billion,
about a quarter of overall spending in Medicare Part D. The table below shows
the various rebate amounts that are required for drugs at different price
points under current law compared with the rebates required under various
discount rates if the rebate were moved to the catastrophic phase with an OOP
threshold of $2,500 (all based on a standard benefit design in 2020).
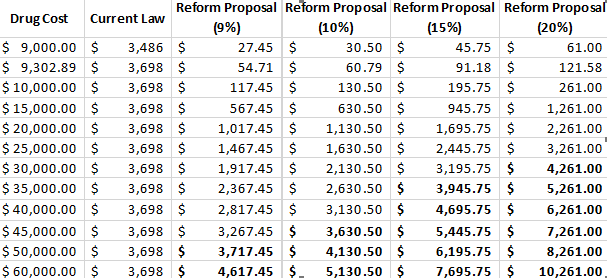
The
bolded numbers in the table highlight costs over (or nearly at) the break-even
price points. As previously stated, if the discount rate is set at 9 percent in
the catastrophic phase, the break-even price is $49,784. If the discount rate
is set at 10 percent, the break-even price drops to $45,675. At 15 percent, the
break-even price is $33,348; and at 20 percent, it is $27,185.
According
to the Centers for Medicare and Medicaid Services (CMS), there were 361 drugs
in 2017 for which average spending per beneficiary for the year exceeded
$8,695, and thus would be required to pay some rebate amount if the mandatory
rebate were moved to the catastrophic phase with a threshold of $2,500.[8] These
drugs were provided to more than 1.5 million beneficiaries at a total cost of
$49.9 billion. An estimated $36.4 billion would have been spent on these drugs
in the catastrophic phase at that threshold. Assuming rebates were required for
all beneficiaries—not just non-low-income subsidy (LIS) beneficiaries as under
current law—a 9 percent rebate on just these drugs would provide $3.3 billion
in mandatory rebates (though this figure does not account for the enrollment
and price growth that has occurred since 2017, nor the drugs that cost less
than $8,695 but will inadvertently be required to pay a rebate simply because
they’re being provided after the beneficiary has reached catastrophic
coverage). If the discount rate was set at 10 percent, the rebates would total
$3.6 billion. At 15 percent, the rebates would equal $5.5 billion, and a 20
percent rate would yield $7.3 billion (again, not accounting for growth in
enrollment, which is expected to increase 10 percent between 2017 and 2020, or
growth in prices since 2017). It is estimated that coverage gap rebates totaled
nearly $6 billion in 2017.[9]
If the
prices for the drugs covered in 2017 increased 5 percent between 2017 and 2020
and the number of beneficiaries increased by 10 percent (the rate that overall
enrollment is expected to have increased during this period), then an
additional 17 drugs provided to an additional 216,000 beneficiaries would be
subject to the rebate. The total estimated spending for these 378 drugs based
on these assumed growth rates would equal $58.2 billion, of which roughly $42.8
billion would occur in the catastrophic phase. A 9 percent discount rate would
yield $3.9 billion in rebates for these drugs. A 10 percent discount rate, $4.3
billion; 15 percent, $6.4 billion; and 20 percent, $8.6 billion. These figures
do not account for any new drugs that have or will come to market since 2017
and that may exceed the threshold.
Milliman
also estimated that if such reforms led to
reductions in brand-name price growth of 5 percent, beneficiaries and the
federal government would see overall savings of $31 billion over 10 years.[10]
Potential
Benefits of Reform
The
benefit structure described here would provide much-needed financial protection
for beneficiaries with high medication costs. The realignment of the
liabilities in the catastrophic phase would encourage both insurers and drug
manufacturers to keep costs down while protecting taxpayers from rising
reinsurance costs. Finally, this change will target the program’s benefits and
mandatory drug rebates more appropriately than the current structure.
[1] In 2020, a beneficiary will reach the
coverage gap after $4,020 in total drug expenditures, of which the beneficiary
will have paid $1,390 in OOP expenses. The beneficiary will exit the coverage
gap after $6,350 in TrOOP costs, $2,652 of which will be paid by the
beneficiary and $3,698 of which will be paid by drug manufacturers if the
beneficiary is taking only brand-name drugs. If the beneficiary is taking just
one drug, then this is the maximum amount a manufacturer would have to pay for
a given drug per beneficiary. (Calculations my own. 2020 plan information found
here: https://q1medicare.com/PartD-The-2020-Medicare-Part-D-Outlook.php)
[2] Schmidt, Rachel and Shinobu Suzuki,
MedPAC. “Options to increase the affordability of specialty drugs and biologics
in Medicare Part D.” April 5, 2019. http://www.medpac.gov/docs/default-source/default-document-library/options-to-increase-the-affordability-of-specialty-drugs-in-pt-d—final.pdf?sfvrsn=0 (Slide
9)
[3] Schmidt, Rachel and Shinobu Suzuki,
MedPAC. “Options to increase the affordability of specialty drugs and biologics
in Medicare Part D.” April 5, 2019. http://www.medpac.gov/docs/default-source/default-document-library/options-to-increase-the-affordability-of-specialty-drugs-in-pt-d—final.pdf?sfvrsn=0 (Slide
9)
[4] Schmidt, Rachel and Shinobu Suzuki,
MedPAC. “Options to increase the affordability of specialty drugs and biologics
in Medicare Part D.” April 5, 2019. http://www.medpac.gov/docs/default-source/default-document-library/options-to-increase-the-affordability-of-specialty-drugs-in-pt-d—final.pdf?sfvrsn=0 (Slide
13)
[5] Schmidt, Rachel and Shinobu Suzuki,
MedPAC. “Options to increase the affordability of specialty drugs and biologics
in Medicare Part D.” April 5, 2019. http://www.medpac.gov/docs/default-source/default-document-library/options-to-increase-the-affordability-of-specialty-drugs-in-pt-d—final.pdf?sfvrsn=0 (Slide
13)
[6] Note that TrOOP includes the rebate
amounts provided by manufacturers. If the manufacturer rebates are moved from
the coverage gap to the catastrophic phase, manufacturer rebates would no
longer count toward a beneficiary’s TrOOP. That is why a lower OOP threshold,
relative to the current TrOOP threshold, is needed to achieve a similar level
of OOP spending directly by the beneficiary.
[7] Based on Milliman’s estimate of rebate
revenues from 2020-2029, under current law, assuming no behavioral
changes. http://us.milliman.com/uploadedFiles/insight/2018/restructuring-Medicare-Part-D-benefit.pdf
[8] Based on average annual spending per
beneficiary, according to the CMS Medicare Part D Drug Spending
Dashboard. https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Information-on-Prescription-Drugs/MedicarePartD.html
[9] https://www.americanactionforum.org/insight/understanding-the-policies-that-influence-the-cost-of-drugs/#_ednref11
https://www.americanactionforum.org/insight/the-impact-of-shifting-rebates-to-catastrophic-coverage-in-medicare-part-d/#ixzz5qf6Ef0V2
Follow @AAF on Twitter
No comments:
Post a Comment