Published: Jun 06, 2019
Since the 1970s, Medicare beneficiaries have had
the option to receive their Medicare benefits through private health plans,
such as HMOs and PPOs, as an alternative to the federally administered
traditional Medicare program. Now called Medicare Advantage plans, these
private health plans receive capitated payments to provide all Medicare-covered
services to plan enrollees. Medicare payments to plans for Medicare Part
A and Part B services are projected to total $250 billion in 2019, accounting
for 33% of total Medicare spending. Over the past decades, Medicare payment policy for
plans has shifted from one that produced savings to one that focused more on
expanding access to private plans and providing extra benefits
to Medicare private plan enrollees across the country. These policy
changes have resulted in more plans offered by more insurers, and enrollment in
Medicare Advantage has increased nationwide.
Medicare Advantage
Enrollment
In 2019, the majority of the 64 million people
on Medicare are covered by traditional Medicare, but one-third
(34%) are enrolled in Medicare Advantage plans (Figure 1). Over the past decade, the number of
beneficiaries enrolled in private plans has nearly doubled from 11.1 million in
2010 to 22.0 million in 2019. Between 2018 and 2019, total Medicare Advantage
enrollment grew by about 1.6 million beneficiaries, or 8 percent – a nearly
identical rate of growth compared to the prior year. The Congressional
Budget Office (CBO) projects that Medicare Advantage enrollment will to
continue to grow over the next decade, with plans including about 47 percent of
beneficiaries by 2029. However, even with an aging Baby Boom Generation, the
majority of new beneficiaries are opting for traditional Medicare in the year
they first go on Medicare, with
29 percent of new Medicare beneficiaries enrolling in Medicare Advantage plans
during their first year on Medicare, as of 2016.
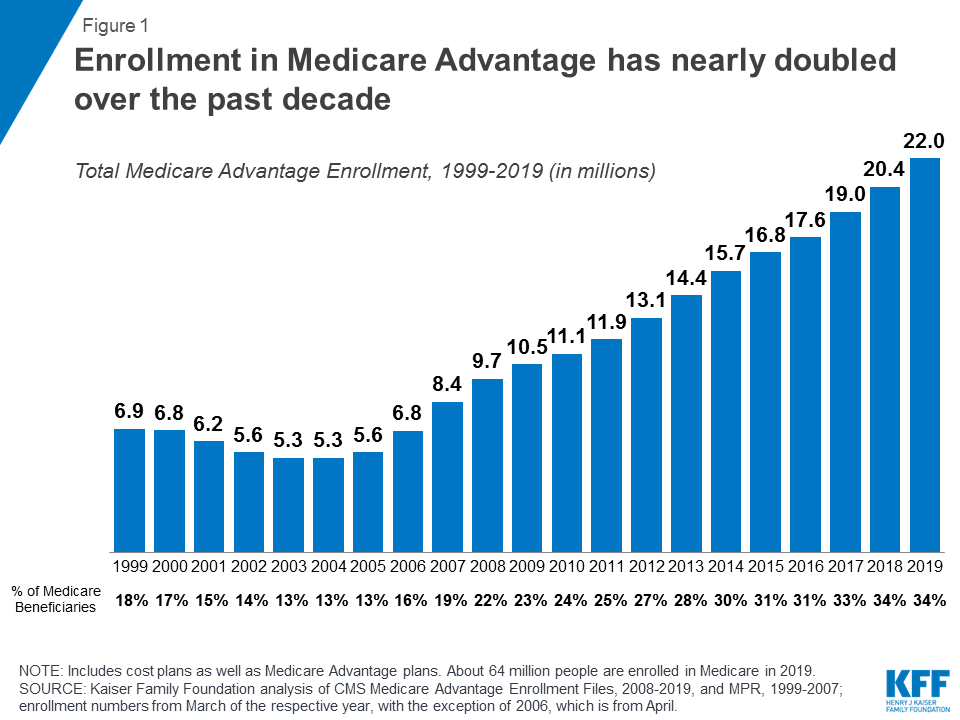
Figure 1: Enrollment in Medicare Advantage has nearly doubled
over the past decade
Medicare Advantage enrollment varies widely
across the states, and by county (Figure 2). In six states (HI, FL, HI, MN, OR, PA, and
WI) and Puerto Rico, more than 40% of Medicare beneficiaries are enrolled in a
Medicare Advantage plan. About one in ten (11%) Medicare beneficiaries live in
a county where the majority of beneficiaries are in a Medicare Advantage plan
in 2019. In 2 states (AK and WY), which are more rural, fewer than 10% of
all beneficiaries are in Medicare Advantage plans.
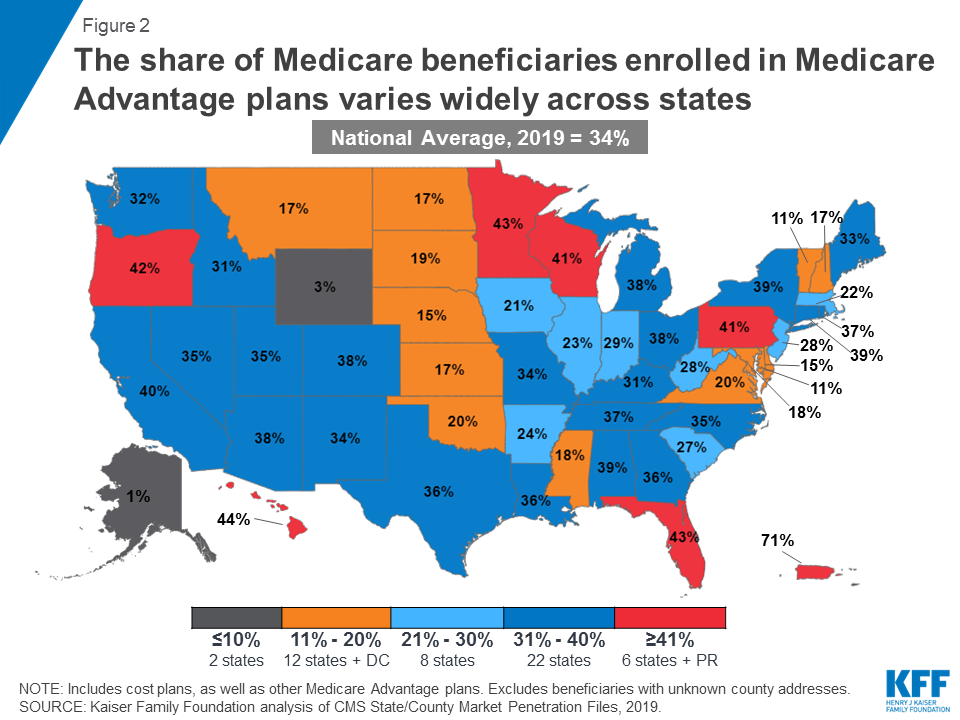
Figure 2: The share of Medicare beneficiaries enrolled in
Medicare Advantage plans varies widely across states
Enrollment continues to be highly concentrated
among a handful of firms, both nationally and in local markets;
UnitedHealthcare and Humana together account for 44% of enrollment in 2019.
Medicare Advantage
Plan Types
Medicare contracts with insurers to offer the
following types of health plans:
HMOs and PPOs are required to establish provider
networks, and HMOs will only cover the services provided by in-network
providers, whereas PPOs cover care delivered by out-of-network providers but
charge enrollees higher cost-sharing for this care. HMOs and local PPOs cover
areas no smaller than a county. Nearly two-thirds (62%) of all Medicare
Advantage enrollees are in HMOs and 31% are in local PPOs in 2019 (Figure 3).
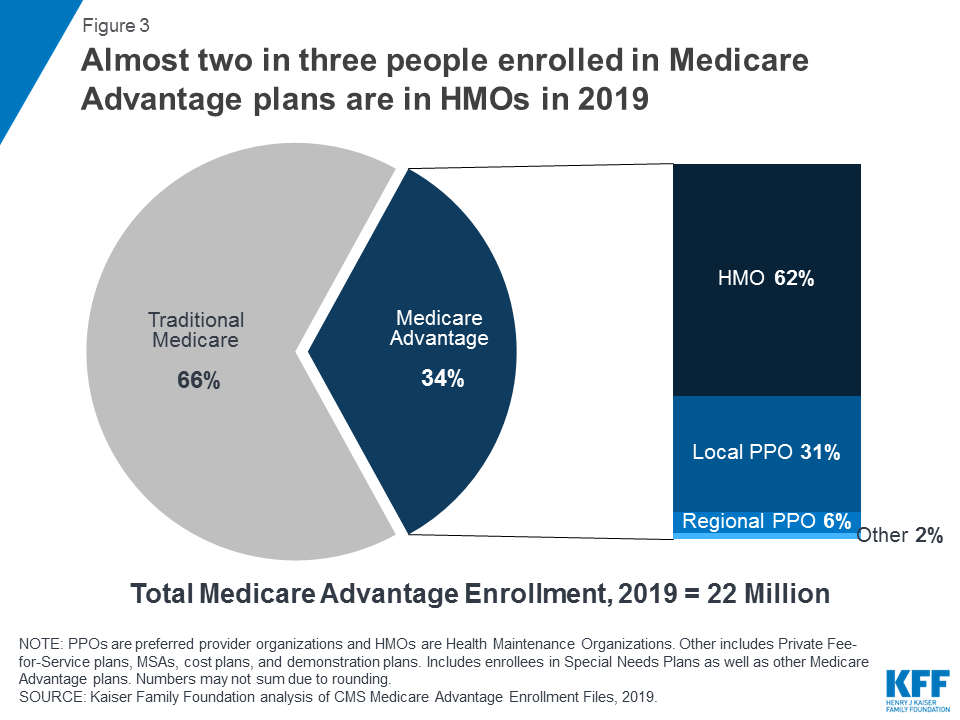
Figure 3: Almost two in three people enrolled in Medicare
Advantage plans are in HMOs in 2019
Regional PPOs were established to provide
rural beneficiaries with greater access to Medicare Advantage plans, including
the extra benefits often covered by the plans, and cover entire statewide or
multi-state regions. Regional PPOs account for 6% of all Medicare Advantage
enrollees in 2019.
Special Needs Plans (SNPs), typically HMOs, are restricted to
beneficiaries who: (1) are dually eligible for Medicare and Medicaid; (2) live
in long-term care institutions or would otherwise require an institutional
level of care; or (3) have certain chronic conditions (Figure 4). In 2019, 2.9 million beneficiaries are
enrolled in SNPs, with plans for dual eligibles accounting for 85% of total SNP
enrollment.
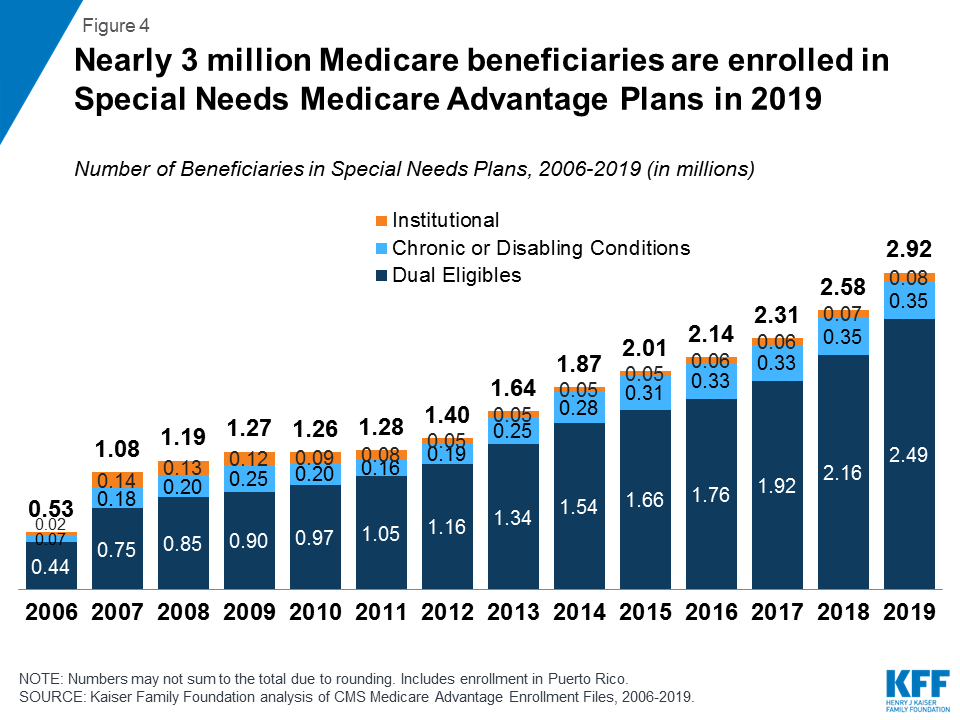
Figure 4: Nearly 3 million Medicare beneficiaries are enrolled
in Special Needs Medicare Advantage Plans in 2019
Group Plans. 4.4 million Medicare Advantage enrollees
(20%) are in a group plan in 2019 – more than double the number of Medicare
beneficiaries in group plans in 2010 (Figure 5). Group plans are largely sponsored by unions
and employers for retirees. Under these arrangements, employers or unions
contract with an insurer to provide Medicare benefits and additional retiree
health benefits to their Medicare-eligible retirees. Medicare pays the insurer
a fixed amount per enrollee to provide benefits covered by Medicare, and the
employer / union, or retiree, pays for any additional benefits. In contrast to
the Medicare Advantage individual market where HMOs dominate, more than
three-quarters (76%) of group plan enrollees are in local PPOs. According to
the 2018
Kaiser Employer Health Benefits Survey, one-third of all large firms
that offer retiree benefits do so through a contract with a Medicare Advantage
plan.

Figure 5: One in five Medicare Advantage enrollees are in
employer or union-sponsored group plans in 2019
Other Plan Types. In addition to HMOs and PPOs, Medicare
contracts with insurers to offer other types of plans, although enrollment in
these other plan types is relatively low. Private Fee-for-Service (PFFS) plans
account for 0.1 million enrollees in 2019, or 1% of all enrollees. In two
states (ND and SD), the majority of private plan enrollment is in cost plans,
which are paid by Medicare based on the “reasonable cost” of providing services
and, unlike Medicare Advantage plans, do not assume financial risk if federal
payments do not cover their costs. In total, about 200,000 Medicare
beneficiaries are enrolled in cost plans in 2019, a decline from the 600,000
enrolled in 2018. Another 43,000 people are enrolled in PACE plans, which are
capitated plans for people over the age of 55 who live in the community but
require an institutional-level of care. A small number of beneficiaries (about
5,600) are enrolled in Medicare Medical Savings Accounts (MSAs) in 2019.
Medicare Payments to
Medicare Advantage Plans
Medicare pays Medicare Advantage plans a
capitated (per enrollee) amount to provide all Part A and B benefits. In
addition, Medicare makes a separate payment to plans for providing prescription
drug benefits under Medicare Part D, just as it does for stand-alone
prescription drug plans (PDPs). Payments to plans are adjusted for enrollees’
health status and other factors.
Over the years, the payment
methodology has been modified to achieve different policy goals, for
example, to attract plans in rural areas, achieve Medicare savings, or deliver
extra benefits to plan enrollees. The Balanced Budget Act (BBA) of 1997
established a payment floor, applicable almost exclusively to rural counties.
The Benefits Improvement and Protection Act (BIPA) of 2000 created payment
floors for urban areas and increased the floor for rural areas. The Medicare
Prescription Drug Improvement and Modernization Act (MMA) of 2003 increased
payments across all areas, and the Affordable Care Act (ACA) of 2010 reduced
payments to plans.
Today, Medicare pays plans based on a bidding
process. Plans submit “bids” based on estimated costs per enrollee for services
covered under Medicare Parts A and B; all bids that meet the necessary
requirements are accepted. The bids are compared to benchmark amounts that are
set by a formula established in statute and vary by county (or region in the
case of regional PPOs). The benchmarks range from 95% of traditional Medicare
costs in the top quartile of counties with relatively high per capita Medicare
costs, to 115% of traditional Medicare costs in the bottom quartile of counties
with relatively low Medicare costs.
If a plan’s bid is higher than the benchmark,
enrollees pay the difference between the benchmark and the bid in the form of a
monthly premium, in addition to the Medicare Part B premium. If the bid is
lower than the benchmark, the plan and Medicare split the difference between
the bid and the benchmark; the plan’s share is known as a “rebate,” which is
designed to be used to provide supplemental benefits to enrollees. Payments to
plans are then adjusted based on enrollees’ risk profiles.
The ACA also established a new system of
bonuses to compensate plans with high quality ratings. Since 2012, Medicare
Advantage plans with 4 or more stars and new plans without ratings have been
receiving bonus payments based on quality ratings. In
2019, 72 percent of Medicare Advantage enrollees are in plans with 4 or more
stars. The ACA also reduced rebates for all plans, but allowed plans
with higher quality ratings to keep a larger share of the rebate than plans
with lower quality ratings.
In 2019, Medicare payments to Medicare
Advantage plans (including bonus payments) are roughly equal to the per capita
costs in traditional Medicare, 100 percent, on average, according to the
Medicare Payment Advisory Commission. The Secretary of Health and Human
Services applies a downward adjustment to payments each year (5.9% in 2019) to
help account for differences in the intensity of coding for health conditions
by Medicare Advantage plans relative to traditional Medicare. Evidence
indicates that beneficiaries who choose to enroll in Medicare Advantage plans
have lower spending and use fewer services – before they enroll
in Medicare Advantage plans – than similar beneficiaries who remain in
traditional Medicare. This suggests that basing payments to plans on
spending of those in traditional Medicare may systematically overestimate the
expected costs of Medicare Advantage enrollees.
Medicare Advantage
Premiums
The average premium for enrollees of Medicare
Advantage plans are $29 per month in 2019, slightly lower than premiums in the
past five years. Average premiums are lower for HMOs than for regional and local
PPOs and significantly vary across counties. However, we do not know to what
extent enrollees’ out-of-pocket expenses have changed since 2010 because we do
not know to what extent cost-sharing for individual services has changed (Figure 6).
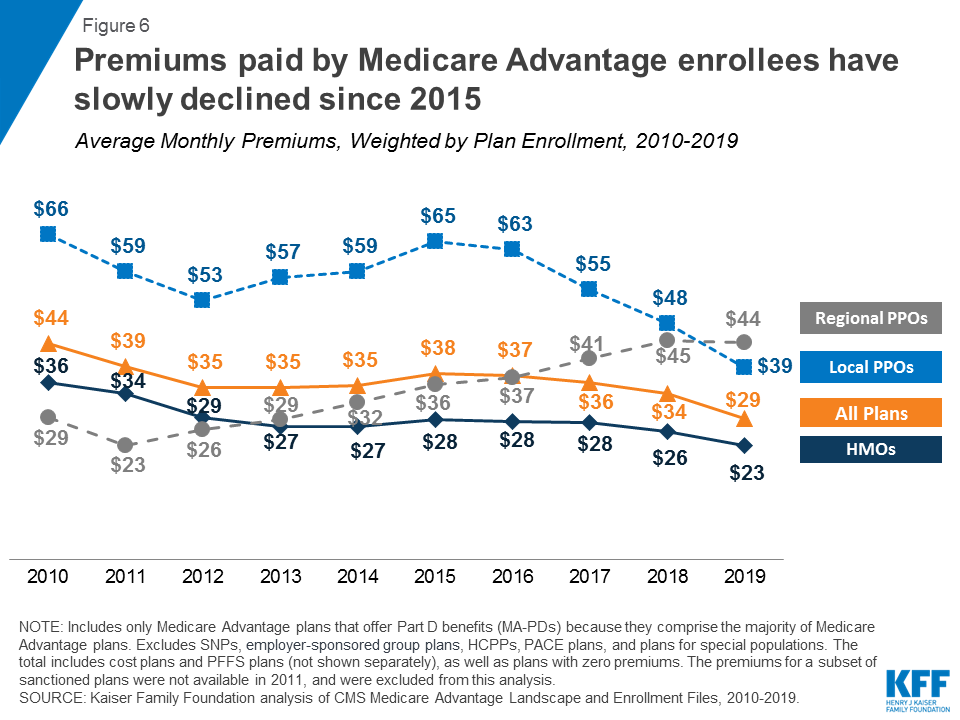
Figure 6: Premiums paid by Medicare Advantage enrollees have
slowly declined since 2015
Supplemental Benefits
Medicare Advantage plans are paid to provide
all Medicare benefits. In addition, since 2011, all plans have been required to
limit beneficiaries’ out-of-pocket spending for services covered under Medicare
Parts A and B to no more than $6,700 (in-network) or $10,000 (in-network and
out-of-network combined). Limits have been required for regional PPOs since
they were first authorized in 2006. Medicare Advantage enrollees’ average
out-of-pocket limit for in-network services is $5,059 (HMOs and PPOs) and $8,818
for out-of-network services (PPOs). (Figure 7).
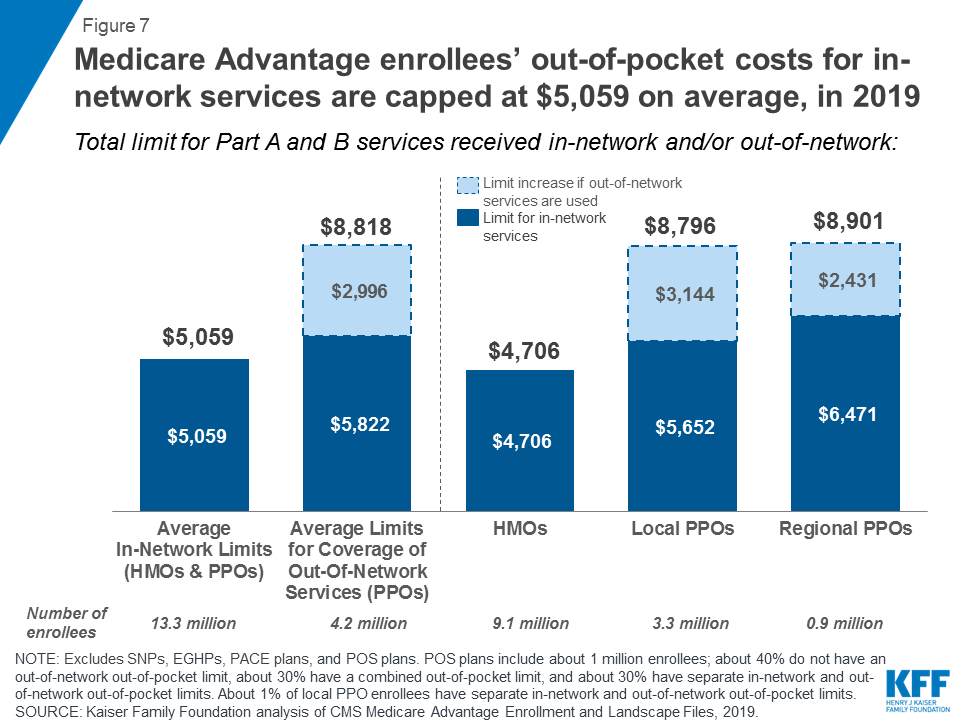
Figure 7: Medicare Advantage enrollees’ out-of-pocket costs for
in-network services are capped at $5,059 on average, in 2019
In addition, plans that receive rebates are
required to use a portion of these payments to provide additional benefits,
reduce premiums, or lower cost sharing for covered benefits. In 2019,
most Medicare Advantage enrollees have access to benefits not covered by
traditional Medicare, and almost eight in ten have access to a dental, fitness,
or vision benefit (Figure 8).
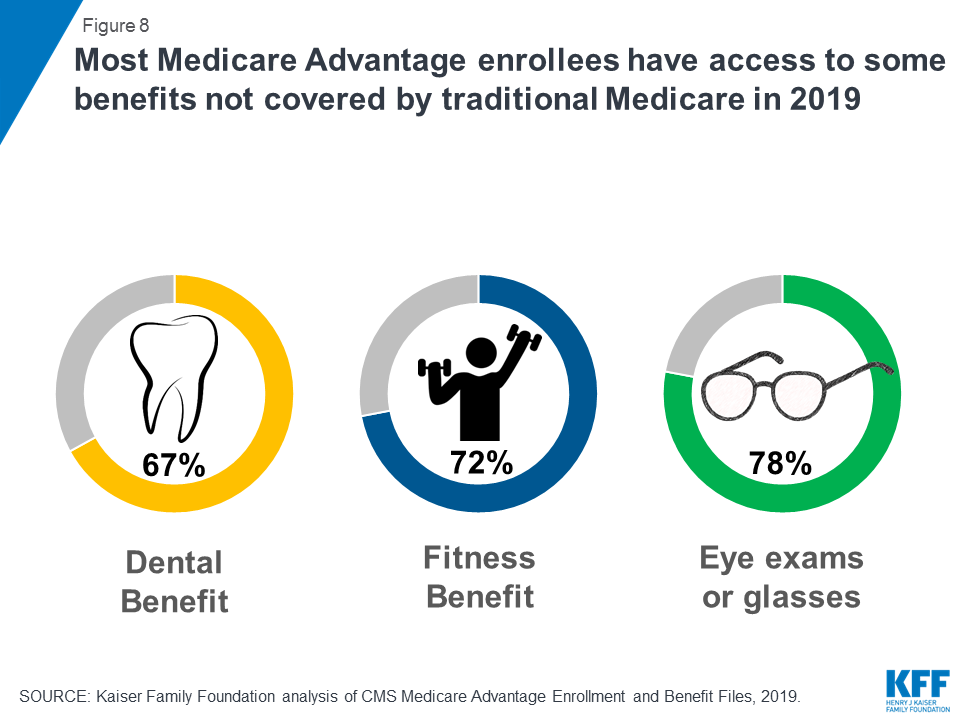
Figure 8: Most Medicare Advantage enrollees have access to some
benefits not covered by traditional Medicare in 2019
Prescription Drug
Benefits
Medicare Advantage plans are generally required
to offer at least one plan that covers the Part D drug benefit. In 2019, 90%
of Medicare Advantage plans offer prescription drug coverage, while
most Medicare Advantage enrollees (88%) select this benefit. In 2019, the
average Part D deductible was $121 for Medicare Advantage plans that offer
prescription drug coverage. The standard Medicare Part D benefit in 2020 will
have a $435 deductible (up from $415 in 2019) and 25% coinsurance up to an
initial coverage limit of $4,020 (up from $3,820 in 2019) in total drug costs,
followed by a coverage gap (enrollees pay 25% of the total costs of brand-name
drugs and 37% of the total costs of generics) until their total out-of-pocket
Part D spending reaches $6,350 (up from $5,100 in 2019) when the catastrophic
limit kicks in and beneficiaries pay 5% of the cost of drugs. The threshold at
which an enrollee reaches the catastrophic threshold increased so significantly
from 2019 to 2020 due to the expiration of the ACA provision that slowed the
growth rate of this threshold between 2014 and 2019.
Medicare Advantage
Provider Networks
Medicare Advantage plans are required to
include a specified number of physicians for each of 26 medical specialties,
plus chiropractic care, along with hospitals, and other providers within a
particular driving time and distance of enrollees in order to ensure that
Medicare Advantage enrollees have access to the physicians that they may need.
Medicare Advantage plan networks have been found to include 51%
of all hospitals in their county and 46%
of the physicians in their county, on average. In 2015, more than
one-third of Medicare Advantage enrollees (35%) were in plans with narrow physician
networks.
Future Issues
Historically, Congress has enacted a number of
changes that affect the role of private plans under Medicare, including adding
new types of plans to the program, increasing or decreasing Medicare payments
to plans, and expanding the types of extra benefits and services that plans can
offer, beyond those included in traditional Medicare.
In 2019, Medicare Advantage markets will have
more companies offering plans and more plans available to beneficiaries
compared to 2018. With new flexibility in plan offerings, utilization
management techniques (such as Part B drug step therapy), and benefits,
companies offering Medicare Advantage plans may respond to payment changes in
several different ways, depending on the circumstances of the company, the
location of their plans, their historical commitment to the Medicare market,
and their quality ratings and bonus payments. Decisions made by these firms
could have important implications for beneficiaries with respect to their
choice of plans, out-of-pocket costs, and access to providers.
Achieving a reasonable balance among multiple
goals for the Medicare program—including keeping Medicare fiscally strong,
setting adequate payments to private plans, and meeting beneficiaries’ health
care needs—will continue to be a critical issue for policymakers in the future.
ALSO
OF INTEREST
No comments:
Post a Comment