Christopher
Holt October 19, 2018
Since the release of President Trump’s “Blueprint to
Lower Drug Prices” this spring, there has been chatter about the Trump Administration requiring drug
manufacturers to publicize the list price of their medications in
direct-to-consumer (DTC) advertising. Sensing that the administration
was ready to move on such a proposal, the Pharmaceutical Research and Manufacturers
of America (PhRMA) preemptively released a
“new approach to DTC television advertising” on Monday promising to provide
more information on drug prices, apparently in the hopes of curtailing action
by the administration.
Nevertheless, later that Monday Health and Human Services Secretary Alex Azar
announced new requirements for
DTC television advertising for prescription drugs that are
available through the Medicare or Medicaid programs. The proposed rule would
require ads to include the list price of the drug advertised. The rule would
allow for either the list price for a 30-day supply or for the typical course
of treatment, whichever is most appropriate. The price must also be current as
of the broadcast date of the ad. Finally, the requirement would not apply to
drugs with a list price of less than $35.
How valuable would
this information be to consumers? There is considerable debate. Critics of the rule argue that list price
is not an appropriate metric, as many consumers do not pay list price for their
drugs. This critique is partially true: Drug pricing is a complicated business,
and an individual’s insurance,
along with other factors, affects the actual price paid. Negotiations
between insurance plans, pharmacy benefit managers, and the manufacturers mean
that the actual price of a drug can vary substantially from the list price.
That said, other considerations suggest such a
rule could benefit consumers. Rising deductibles mean more Americans are paying the full cost of
their drugs, at least for a time. Additionally, most insured individuals
pay coinsurance on their drugs even after reaching their deductible.
Coinsurance is a percentage of the cost of the medication, and it is often
based on the list price, even if the insurer has negotiated a lower price. In
those cases, list price can be helpful in determining the cost to the consumer.
A second point of contention is whether the
Centers for Medicare and Medicaid Services (CMS) has the authority to require
the disclosures at all. The Food and Drug Administration regulates drug
advertising, but CMS is proposing this rule. In effect, CMS is saying, “As the
largest purchaser of your product, we demand you comply with this proposal.” To enforce the rule, CMS will publish a list
of companies who fail to comply, apparently in hopes of shaming manufacturers
into going along with the rule. While that penalty might seem weak, it’s
not obvious what penalties the agency could legally impose, short of refusing
to purchase specific medications (which they are considering and seeking
comment on). Limiting access to specific drugs has long been a political
nonstarter—it’s part of why direct
negotiations by the HHS secretary over drug prices wouldn’t
have much effect.
The president has made it clear he wants to
force companies to lower their prices, but the federal government has limited
legal mechanisms for accomplishing his goal. If implemented, this proposal probably won’t significantly
affect drug purchasing decisions. It could, however, increase public awareness about drug prices.
CHART REVIEW
Jonathan Keisling, Health Care Policy Analyst
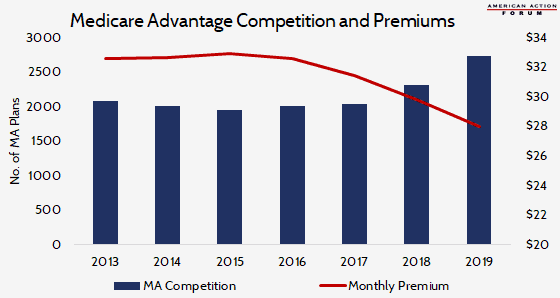
Last week in the Weekly Checkup,
Tara Hayes noted that the Medicare Advantage (MA) program’s enrollment is
increasing while premiums are decreasing, but why are MA premiums decreasing?
One reason why MA premiums have fallen in recent years could be the uptick in
competition among MA plans. The total number of MA plans available in 2019 will
mark a 10-year high.
https://www.americanactionforum.org/weekly-checkup/the-shaming-of-big-pharma/#ixzz5UfRvY7wG
Follow: @AAF on Twitter
No comments:
Post a Comment