September 10, 2020 Tara O'Neill Hayes, Serena Gillian
Executive Summary
·
The prevalence and cost
of chronic disease in the United States is growing and will continue to grow,
not just as a result of the Baby Boomer generation aging but also due to
increased disease prevalence among children and younger adults.
·
The prevalence of
chronic disease varies greatly across the country with a higher concentration
in the Mid-South region.
·
Those with chronic
disease and their families face both direct and indirect costs: Direct costs
primarily stem from longer and more frequent hospital visits and greater
prescription drug use, while indirect costs arise from lost education and job
opportunities.
·
When including indirect
costs associated with lost economic productivity, the total cost of chronic
disease in the United States reaches $3.7 trillion each year, approximately
19.6 percent of the country’s gross domestic product.
Introduction
Chronic
disease in the United States, already highly prevalent, is expected to worsen
over the next several decades among all age groups. The burden of the
associated physical and economic costs will worsen, as well. But the burdens of
chronic disease do not just loom in the future: Evidence suggests that the high
prevalence of chronic disease may be partially responsible for the devastating
effects of the current coronavirus pandemic.[1] Further, the economic
consequences of the pandemic have made it even more difficult
for the United States to afford the growing health care costs that result from
chronic disease.
A
disease is considered chronic when it persists for at least a year and requires
ongoing medical attention or limits daily activities.[2] Approximately 45 percent of the U.S.
population, 133 million Americans, suffer from at least one chronic disease.[3] Almost 30 million Americans are
living with five or more chronic diseases.[4] The risk and prevalence of chronic
disease grows as individuals age. Approximately 27 percent of children in the
United States suffer from a chronic condition, while about 6 percent of
children have more than one chronic condition.[5] In contrast, around 60 percent of
adults suffer from at least one chronic condition, while 42 percent suffer from
multiple conditions.[6] Among those 60 or older, at least 80
percent have one chronic illness and 50 percent have two.[7] These ailments account for 70
percent of all deaths in America, killing more than 1.7 million people each
year.[8]
The
share of health care costs borne by those with chronic disease are
disproportionate to the number of people affected. An estimated 84 percent of
health care costs are attributed to the treatment of chronic disease.[9] The rates are even higher for
beneficiaries in public health insurance programs: 99 percent of Medicare and
80 percent of Medicaid spending went toward the treatment of chronic diseases,
as of 2010.[10] Given the correlation between
chronic disease and age, this health and cost burden is only expected to grow:
It’s estimated that by 2060, the U.S. population aged 65 years and older will
more than double, from 46 million today to 98 million.[11]
Change in Prevalence Over Time
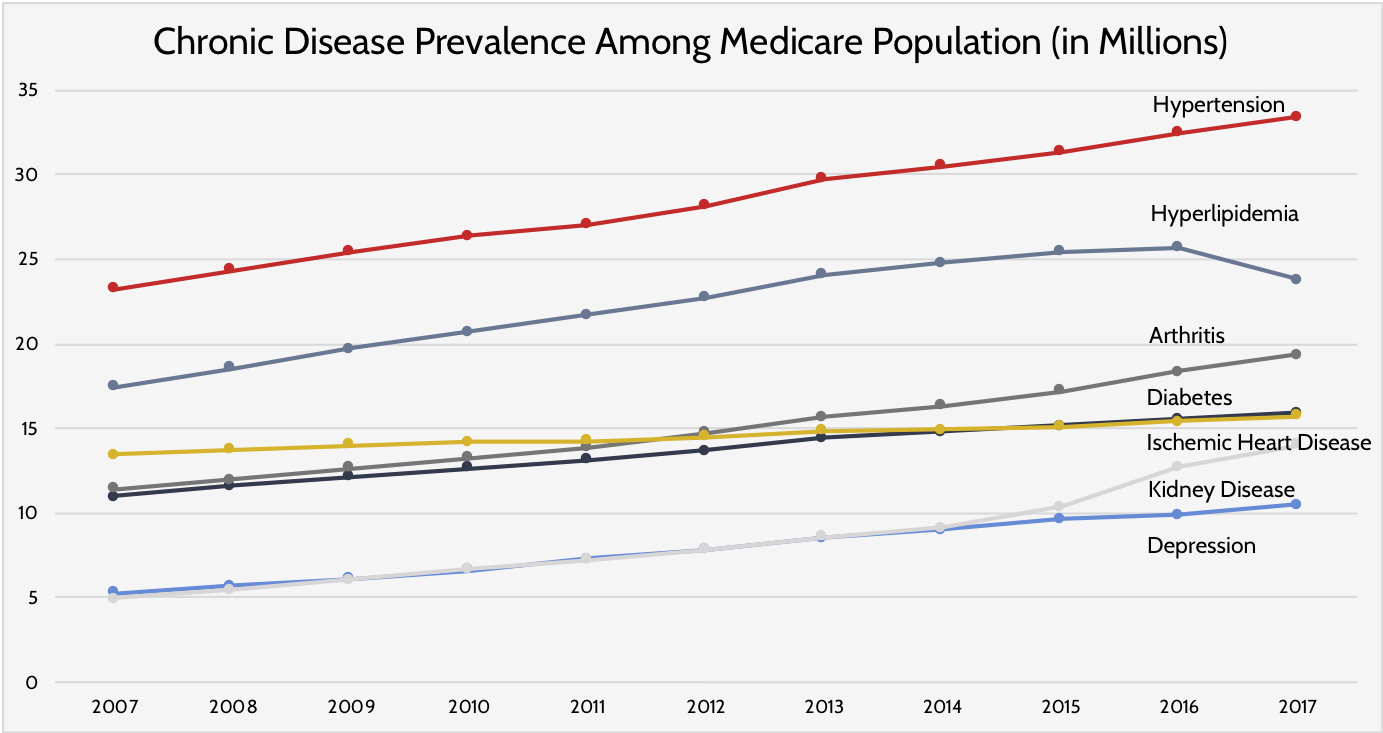
The
growth in the number of individuals with chronic diseases is likely to continue
at the same trajectory as existing trends shown. As shown in Figure 1, the
number of Medicare beneficiaries suffering from any of the diseases defined as
“chronic” by the Centers for Medicare and Medicaid Services (CMS), other than
hyperlipidemia (resulting from high levels of fat particles (lipids) in the
blood), has grown steadily from 2007 to 2017.[12]
Figure
1:
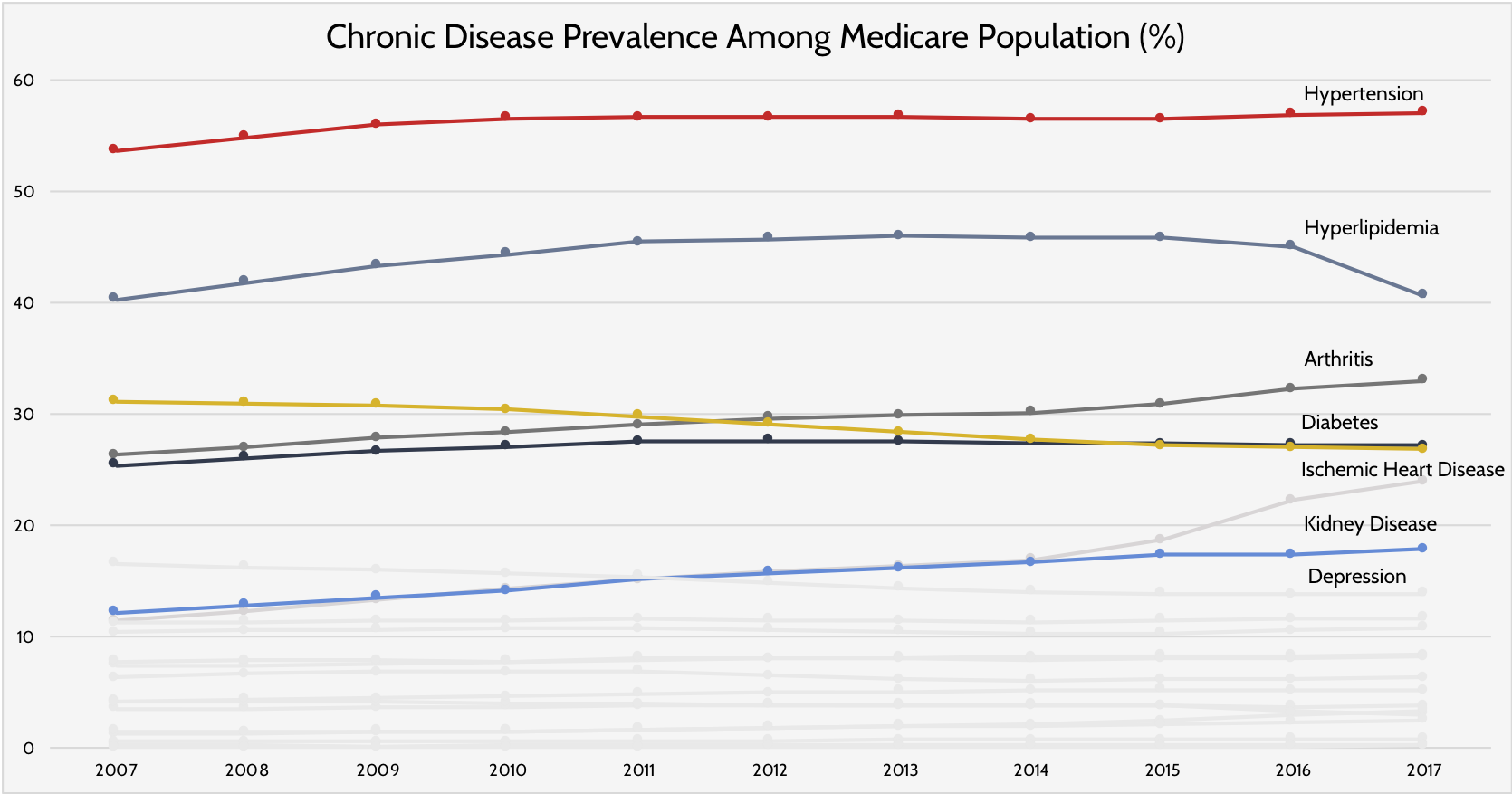
It
does not appear, however, that this growth is driven by a heightened prevalence
of chronic disease but rather a growth in the population that is most affected
by it. This distinction can be seen in Figure 2. With the exception of kidney
disease, arthritis, and depression, the proportion of the Medicare population
suffering from chronic disease has not grown significantly, while the
prevalence of some diseases has even decreased.[13] These trends imply that the risk of
chronic disease is not growing among this population.
Figure
2:
While
the risk of chronic disease is not growing among older adults, the incidence
among older adults is, and this growth is not just occurring in this
demographic. A recent study comparing the prevalence of 17 chronic
diseases among various age groups between 2005 and 2014 found increases in
nearly every disease, including in the youngest groups in the study: 35-50
years old and 51-65 years old.[14] Children have similarly suffered
from increasing rates of chronic disease. Less than 2 percent of children in
1960 had a health condition severe enough to interfere with activities of daily
life; 50 years later, more than 8 percent of children had such a condition.[15] Much of the increase is associated
with greater prevalence of four types of conditions: asthma, obesity, mental
health conditions, and neurodevelopmental disorders (which affect brain
developmental and may result in neuropsychiatric problems or impaired motor
function, learning, or communication skills).[16] In the last three decades, the
prevalence of obesity has more than doubled in children and tripled in
adolescents, reaching nearly 19 percent overall as of 2016.[17] Between 2001 and 2009, the
prevalence of juvenile diabetes increased 23 percent.[18] In 2012, University of Michigan
estimated that between 15 to 18 percent of children had at least one chronic
condition.[19]
Geographic Variation
Although
chronic disease affects approximately half of the U.S. population, there are
parts of the country facing a far higher burden than others. Figure 3 displays
the distribution of chronic disease among Medicare beneficiaries in the United
States. Each state has been given its own average chronic disease prevalence
value, calculated by summing the proportions of Medicare beneficiaries
suffering from each of 21 different chronic diseases in a state and dividing
the sum by 21, the total number of chronic diseases measured.[20]
Figure
3:
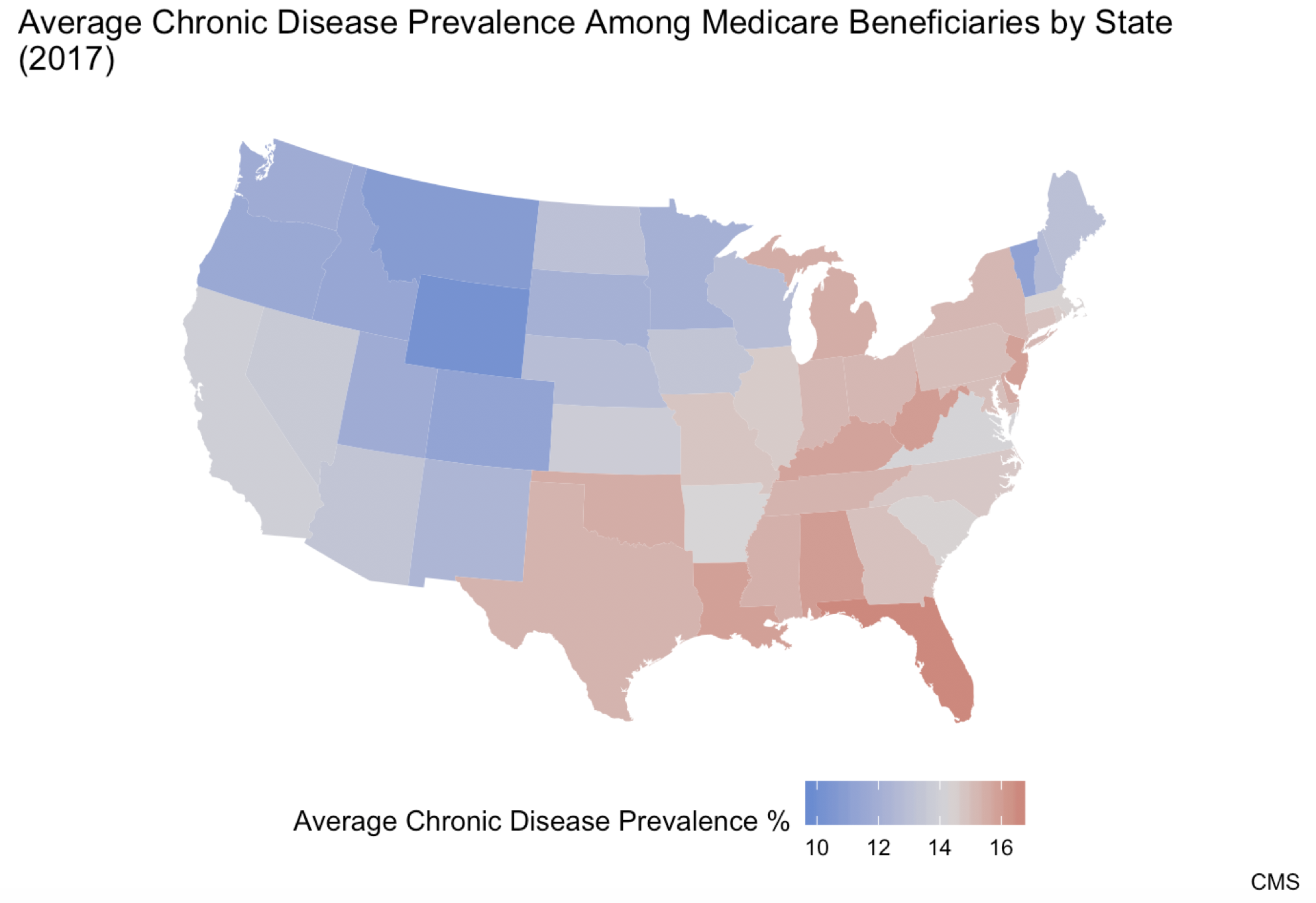
As
seen above, the highest prevalence of chronic disease is concentrated in the
Mid-South region. The state with the highest average chronic disease
prevalence—16.6 percent—is Florida. The state with the lowest average chronic
disease prevalence is Wyoming at 9.8 percent. Note that because these
prevalence rates are based on the percentage of the Medicare
population with a given disease within each state, Florida’s prevalence rate is
not higher simply because it is home to a larger share of Medicare
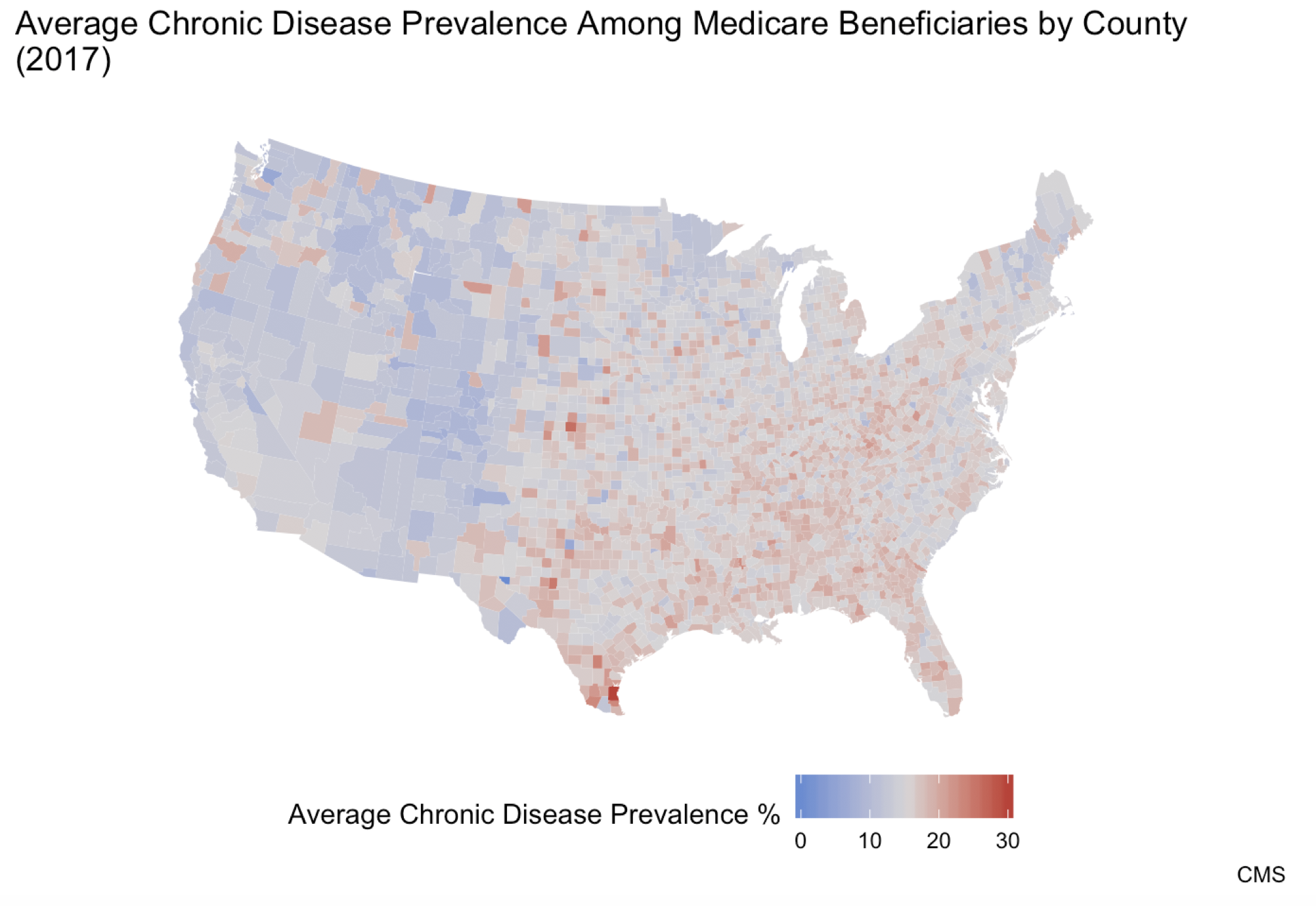
beneficiaries than other states. It’s also important to note that within the
states, there is even further variation at the county level, as shown in Figure
4. The county with the highest average chronic disease prevalence is Kenedy
County, Texas with a disease prevalence of 30.0 percent. Multiple counties
share the status of lowest prevalence with an average chronic disease
prevalence of 0.0 percent, including Loving County, Texas. This goes to show
the degree of variation that can exist within a single state.
Figure
4:
Mechanisms
driving this geographic variation include social
determinants such as income, education, and health care access,
as well as the racial makeup of a given area. In states and counties with
higher proportions of minorities, chronic disease is often more prevalent,
driven by a multitude of factors.
Costs
The
costs associated with chronic disease in the United States, both direct and
indirect, are immense. Direct costs are those attributed to the prescriptions,
procedures, and other health care products and services needed to treat
individuals with chronic diseases. Indirect costs are those associated with the
impacts of chronic disease in other realms of life, such as effects on
employment, mobility, and other factors associated with well-being. When
including indirect costs associated with lost economic productivity, the total
cost of chronic disease in the United States reaches $3.7 trillion each year,
approximately 19.6 percent of the country’s gross domestic product.[21] Like chronic disease prevalence,
chronic disease costs also vary greatly between states.
Direct Costs
The
health care costs of individuals with chronic disease tend to dwarf those of
individuals without a chronic disease. Annually, direct health care costs for a
patient with chronic disease average $6,032, approximately 5 times that of a
person without a chronic disease.[22] These costs are primarily derived
from more frequent hospitalizations and emergency room visits and greater
prescription drug use.
The
Milken Institute estimates costs associated directly with chronic disease
totaled $1.1 trillion in 2016, with cardiovascular conditions accounting for
26.7 percent of costs, followed by diabetes with 17.2 percent of costs,
Alzheimer’s accounting for 16.9 percent, and Arthritis and back pain accounting
for 16.5 percent of costs.[23] Obesity—the greatest single risk
factor for chronic disease—is responsible for nearly 44 percent of direct
health care costs.[24]
Hospitalizations
More
frequent and longer lengths of stay are the drivers of higher hospitalization
costs for individuals with chronic disease.[25] While only 3 percent of individuals
with no chronic disease had an inpatient hospital stay in 2014, 10 percent of
those with 3-4 chronic conditions and 24 percent of those with 5 or more did.[26] The length of one’s hospital stay
is similarly impacted by the existence of chronic disease. Compared to those
with 0 or 1 chronic condition, acute condition stays are 11 percent longer for
those with 2 or 3 chronic conditions, 21 percent longer when 4 or 5 conditions
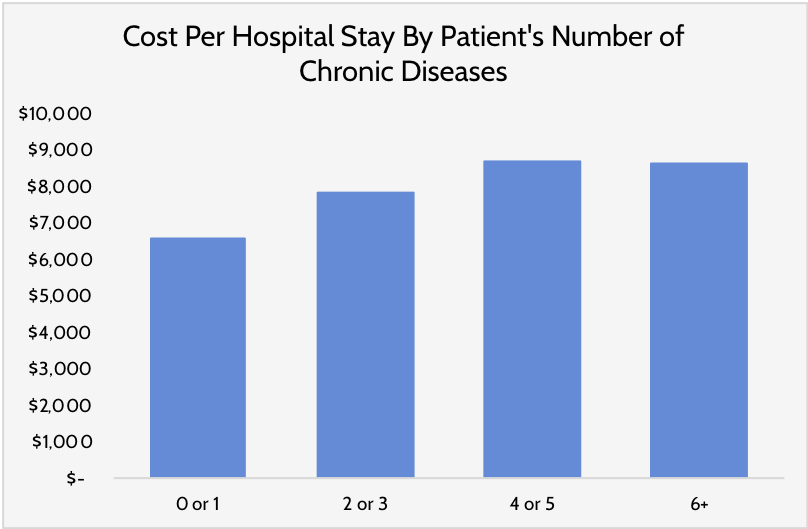
are present, and 27 percent longer when 6 or more conditions are present.[27] The same pattern applies to stays
associated with a chronic disease itself, as well as associated costs. For
example, relative to patients with 0 or 1 conditions, costs per stay for
ambulatory-care-sensitive conditions (those for which effective outpatient care
can reduce the likelihood of hospitalization) were 19 percent higher for those
with 2 or 3 chronic conditions, 32 percent higher for those with 4 or 5, and 31
percent higher for those with 6 or more, as shown in Figure 5.[28]
Figure
5:
Prescriptions
Individuals
with chronic disease have greater prescription drug costs.[29] This higher cost is mostly due to
the sheer number of prescriptions taken: In 2014, people with no chronic
conditions took an average of 1 prescription per year while people with 3-4 chronic
conditions took 24 and those with 5 or more conditions used 51 or more.[30] The high costs associated with the
higher number of prescriptions can lead to non-adherence among patients as a
strategy for reducing costs which often ultimately worsens health outcomes and
increases the potential for an expensive hospitalization.[31] In fact, the Congressional Budget
Office recently noted that for each dollar of improved medication adherence,
medical costs are reduced by $2.00.[32] Poor medication adherence is
particularly prevalent among seniors given that they are more likely to suffer
from chronic disease, have multiple prescriptions, and have lower incomes. A
number of experts argue that the standard practice of treating each chronic
condition individually leads to over-prescription and sometimes harmful
interaction, and as a result changing treatment practices could result in lower
costs, better adherence, and fewer complications.[33]
Emergency Room Visits
Nearly
60 percent of all emergency room visits are associated with people with chronic
conditions, at a cost of $8.3 billion in 2017.[34] It’s estimated that nearly 30
percent of such visits could be prevented or treated in a lower-cost setting if
better managed.[35] The financial toll of these
preventable visits is estimated at $2.5 billion.[36] People with chronic diseases
inappropriately use the emergency room for a number of reasons. People often
lack the knowledge needed to manage their disease, use their medications
improperly, are unable to engage in effective self-care, fail to adhere to
their treatment plan, or lack access to other forms of medical care.[37] For example, diabetes patients
without health insurance have 168 percent more emergency department visits than
their insured counterparts.[38] At the root of such overuse is a
lack of understanding and appreciation for the importance of using alterative
care settings, insufficient income necessary to keep oneself healthy, and, at
times, mental health challenges.
Indirect Costs
Chronic
disease creates costs far beyond medical care. Individuals with chronic disease
can see their lives impacted in ways that are difficult to measure objectively
but are potentially devastating nonetheless. Chronic disease affects people’s
education, their livelihoods, and even social interaction. These consequences
impact the overall welfare of those with a disease and their families, as well
as society at large. In fact, the indirect costs of some diseases far outweigh
the direct costs: the indirect cost of hypertension is estimated at 14.7 times
the direct cost; prostate cancer, 6.8 times; chronic back pain, 5.7;
osteoarthritis, 2.5; Type 2 Diabetes, 1.8.[39] One study estimates that the total
cost of chronic conditions, after accounting for indirect costs, will total $42
trillion between 2016 and 2030, nearly 40 percent of which will be the result
of lost employee productivity, as discussed below.[40]
Education and Human Capital
Chronic
disease can interfere with the educational attainment of those who have a
disease and their families. The spending required to treat a chronic disease
has the potential to crowd out investing in higher education, a key determinant
for future earnings.[41] Since low-income families often
face a higher chronic disease burden, the increased costs associated with
chronic disease make it even more difficult for children in these families to
achieve upward economic mobility and thus, low-income families face a higher
possibility of becoming entrenched in poverty. Chronic diseases such as
addiction can affect a child’s future before they’re born. For example, smoking
during pregnancy has been shown to impair a child’s cognitive and behavioral
development and correlates with reduced human capital formation and
productivity later in life.[42] People with a chronic disease are
also more at risk for a premature death, an event that can severely impact
their children’s educational attainment. Studies have shown that a child whose
parent has recently died is twice as likely to drop out of school than children
whose parents are still alive.[43]
Children
also suffer educationally when they themselves have a chronic disease.
Overweight or obese children struggle more in school than their peers due to
the effects of their disease. They are often more likely to miss school,
exhibit low self-esteem, and feel more shame.[44] These experiences are all
significant obstacles to learning. Beyond learning, the essential social skills
directly and indirectly taught in schools are highly valuable later in life.
Chronic diseases that require careful monitoring, such as diabetes, can reduce
children’s ability to fully participate at school and leave them feeling
isolated in non-classroom settings such as recess and lunch.
Economic Well-Being
Having
a chronic disease can often prevent people from having the financial resources
they need to thrive. Due to chronic disease, individuals may lose the ability to
perform their job duties to the extent that is expected. This effect is felt
especially by people in low-paying jobs, which often require physical labor and
allow for few, if any, days of leave.[45] Absences from work caused by
chronic disease can result in reduced income or complete job loss.[46] Since the burden of care for those
with chronic disease can often fall on relatives, their own productivity and
income may fall as well.[47] Additionally, because of the
aforementioned challenges for people with chronic diseases in getting an
advanced education, such individuals may be less likely to get a high-paying
job.
In
more severe cases, chronic disease can prevent people from entering the labor
force in the first place. One study conducted in Australia using data from the
Australian National Health Survey found that labor force participation dropped
by 3.9 percent for diabetic young men (aged 18-49) and 11.4 percent for
diabetic older men (aged 50-64) when compared to their counterparts with no
chronic disease.[48] This effect became more pronounced
as subjects aged and suffered from more chronic diseases. For example, older
men with four chronic diseases were employed at a rate of just 27.8 percent,
whereas those without a chronic disease participated at a rate of 81.3 percent.[49]
The
impacts of these consequences are significant and reach far beyond the
individuals living with the disease: Labor productivity and labor force
participation are the two key determinants of a country’s economic output.[50] Low productivity is associated with
falling wages.[51] Low labor force participation rates
are associated with slower economic growth, a higher dependency ratio, and
higher tax rates.[52]
Social Well-Being
The
disabilities associated with and the monitoring required for chronic diseases
can be socially debilitating for many. Mental and physical chronic conditions
can lead to harmful degrees of social isolation. Mobility restrictions and
mental difficulties can make interacting with others difficult. Social
isolation has been shown to have devastating effects on physical and mental
health, as well, perpetuating a cycle of isolation and declining health.[53] When considering the
vulnerabilities of people with chronic disease, the indirect effects of social
isolation are important to understand. It has been shown that those who report
frequent feelings of loneliness or who lack social connections suffer higher
rates of morbidity and mortality, infection, depression, and cognitive decline.[54] Someone who is chronically ill and
socially isolated may be less likely to adhere to their treatment regimen and,
as a result, become more ill.
Conclusion
Chronic
disease and its associated costs continue to climb in the United States, across
all age groups. Given that the increased prevalence is not limited to elderly
Americans, the burden of chronic disease will plague this country for many
decades to come. Higher medical costs and a lower capacity to participate in
the labor force or earn a livable wage as a result of chronic disease may
worsen a person’s quality of life and, often, that of their family members,
resulting in significant indirect costs. These effects persist and often worsen
over time. The costs associated with chronic disease also place significant
financial burdens on public resources and hinder economic growth. As the number
of individuals with chronic disease grows, this burden will grow as well.
Low-income individuals are more likely to suffer from chronic disease and may
be disproportionately burdened by the costs and associated social and economic
consequences. Interventions to prevent and better manage existing chronic
disease can reduce direct costs and prevent many indirect costs from ever
emerging, thus improving the economic well-being of individuals and the country
as a whole.
[1] https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html
[2] https://www.cdc.gov/chronicdisease/about/index.htm#:~:text=Chronic%20diseases%20are%20defined%20broadly,disability%20in%20the%20United%20States.
[3] https://www.fightchronicdisease.org/sites/default/files/docs/GrowingCrisisofChronicDiseaseintheUSfactsheet_81009.pdf
[4] https://www.rand.org/blog/rand-review/2017/07/chronic-conditions-in-america-price-and-prevalence.html
[5] https://www.cdc.gov/pcd/issues/2015/14_0397.htm#:~:text=Approximately%2027%25%20of%20children%20in,this%20population%20have%20been%20limited.
[6] http://www.fightchronicdisease.org/sites/default/files/TL221_final.pdf
[7] https://www.cswe.org/getattachment/Centers-Initiatives/Gero-Ed-Center/Initiatives/Past-Programs/MAC-Project/Resource-Reviews/Health/CI-Sec1-Demographics.pdf.aspx#:~:text=At%20least%2080%25%20of%20people,illnesses%20(CDC%2C%202003).
[8] https://www.fightchronicdisease.org/sites/default/files/docs/GrowingCrisisofChronicDiseaseintheUSfactsheet_81009.pdf
[9] https://www.rwjf.org/en/library/research/2010/01/chronic-care.html
[10] https://www.rwjf.org/en/library/research/2010/01/chronic-care.html
[11] https://milkeninstitute.org/sites/default/files/reports-pdf/ChronicDiseases-HighRes-FINAL.pdf
[12] The
remaining diseases not included in the figure showed a constant prevalence over
the years.
[13] The
unlabeled lines at the bottom represent the remaining diseases that follow the
trend.
[14] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6351821/
[15] https://www.healthaffairs.org/doi/full/10.1377/hlthaff.2014.0832
[16] https://www.healthaffairs.org/doi/full/10.1377/hlthaff.2014.0832
[17] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6887808/
[18] https://www.focusforhealth.org/chronic-illnesses-and-the-state-of-our-childrens-health/
[19] http://www.med.umich.edu/yourchild/topics/chronic.htm
[20] The
percentages are the percentage of Medicare beneficiaries in the state suffering
from a chronic disease. So, 14 percent diabetes in Colorado means that 14
percent of the Medicare beneficiaries in Colorado have been diagnosed with
diabetes. The average disease score for each state was determined by averaging
all the percentages for each disease within that state. For example, if only
three diseases were being measured, and in Florida 2 percent of beneficiaries
suffered from alcoholism, 20 percent from diabetes, and 15 percent from
Alzheimer’s, the disease score for the state would be (2 percent + 20 percent +
15 percent )/ 3 = 12.3 percent.
[21] https://milkeninstitute.org/sites/default/files/reports-pdf/ChronicDiseases-HighRes-FINAL.pdf
[22] https://cdn.ymaws.com/www.chronicdisease.org/resource/resmgr/white_papers/cd_white_paper_hoffman.pdf
[23] https://milkeninstitute.org/sites/default/files/reports-pdf/ChronicDiseases-HighRes-FINAL.pdf
[24] https://milkeninstitute.org/sites/default/files/reports-pdf/ChronicDiseases-HighRes-FINAL.pdf
[25] https://www.hcup-us.ahrq.gov/reports/statbriefs/sb183-Hospitalizations-Multiple-Chronic-Conditions-Projections-2014.pdf
[26] http://www.fightchronicdisease.org/sites/default/files/TL221_final.pdf
[27] https://bmchealthservres.biomedcentral.com/articles/10.1186/s12913-016-1304-y
[28] https://bmchealthservres.biomedcentral.com/articles/10.1186/s12913-016-1304-y
[29] https://gh.bmj.com/content/bmjgh/3/1/e000505.full.pdf
[30] http://www.fightchronicdisease.org/sites/default/files/TL221_final.pdf
[31] https://gh.bmj.com/content/bmjgh/3/1/e000505.full.pdf
[32] https://www.cbo.gov/system/files/2019-05/55151-SupplementalMaterial.pdf
[33] https://gh.bmj.com/content/bmjgh/3/1/e000505.full.pdf
[34] https://healthitanalytics.com/news/chronic-conditions-account-for-8.3b-in-avoidable-ed-visits
[35] http://offers.premierinc.com/rs/381-NBB-525/images/Improving
Care for Chronic Conditions, Premier.pdf
[36] http://offers.premierinc.com/rs/381-NBB-525/images/Improving
Care for Chronic Conditions, Premier.pdf
[37] http://offers.premierinc.com/rs/381-NBB-525/images/Improving
Care for Chronic Conditions, Premier.pdf
[38] http://offers.premierinc.com/rs/381-NBB-525/images/Improving
Care for Chronic Conditions, Premier.pdf
[39] https://milkeninstitute.org/sites/default/files/reports-pdf/ChronicDiseases-HighRes-FINAL.pdf
[40] https://www.fightchronicdisease.org/sites/default/files/pfcd_blocks/PFCD_US.FactSheet_FINAL1%20(2).pdf
[41] https://www.who.int/management/programme/ncd/Chronic-disease-an-economic-perspective.pdf?ua=1
[42] https://www.who.int/management/programme/ncd/Chronic-disease-an-economic-perspective.pdf?ua=1
[43] https://www.who.int/management/programme/ncd/Chronic-disease-an-economic-perspective.pdf?ua=1
[44] https://www.who.int/management/programme/ncd/Chronic-disease-an-economic-perspective.pdf?ua=1
[45] https://www.americanactionforum.org/research/the-outsized-impact-of-the-coronavirus-pandemic-on-minority-communities/
[46] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4493930/
[47] https://www.who.int/chp/chronic_disease_report/part2_ch2/en/index7.html
[48] https://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.175.5777&rep=rep1&type=pdf
[49] https://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.175.5777&rep=rep1&type=pdf
[50] https://www.spglobal.com/en/research-insights/articles/declining-labor-force-participation-will-weigh-on-us-gdp-growth-and-fed-monetary-policy
[51] https://opentextbc.ca/principlesofeconomics2eopenstax/chapter/labor-productivity-and-economic-growth/
[52] https://www.bls.gov/opub/mlr/2018/beyond-bls/down-and-down-we-go-the-falling-us-labor-force-participation-rate.htm
[53] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2756979/
[54] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2756979/
Disclaimer
https://www.americanactionforum.org/research/chronic-disease-in-the-united-states-a-worsening-health-and-economic-crisis/#ixzz6Xk88hRns
Follow @AAF on Twitter
This comment has been removed by a blog administrator.
ReplyDelete