Tara
O'Neill Hayes June 28, 2019
Executive Summary
AAF’s proposal to reform the Medicare
Part D program has gained attention recently, but with this attention have come
both questions and suggestions for how the proposal could be modified. This
paper discusses some of those ideas and provides further analysis to better
inform the conversation.
·
In setting an
out-of-pocket (OOP) cap, the primary trade-off to consider is how many
beneficiaries should receive financial protection versus how much premiums
should be increased: the lower the OOP cap, the higher the premiums.
·
Requiring drug
manufacturers to pay rebates in coverage phases beyond just the catastrophic
phase will more evenly spread the burden across manufacturers and drug classes,
but may weaken the incentive not to increase prices, relative to AAF’s original
proposal, depending on the discount rates required. It may also provide
financial savings to more beneficiaries.
·
Implementing this
proposal in combination with the administration’s proposed “rebate rule” could
lead to even higher premium increases. Further, a lower OOP cap would be
required to keep the overall spending that occurs before catastrophic coverage
at roughly the same level, which in turn would keep expected manufacturer
rebates roughly equal.
Potential Modifications to AAF’s Proposal
AAF’s proposal seeks to address a couple of
problems in the current structure of Medicare Part D. Because insurer liability
is very limited in the catastrophic phase, insurers have little incentive to
keep beneficiaries out of that final phase. Further, drug manufacturers have no
real incentive to keep their prices down. The result of this lack of incentives
is that the government is paying more of Part D’s cost in the catastrophic
phase, and the government’s overall costs are rising. Finally, the current
structure leaves some beneficiaries with very high costs even in the
catastrophic phase.
AAF’s proposal addresses these problems by
making several changes: It increases insurer liability in the catastrophic
phase, moves the required manufacturer rebates to the catastrophic phase, and
places a cap on beneficiaries’ out-of-pocket (OOP) liability. There are several
provisions of the proposal which could be modified—to a degree—without
substantially undermining the intent of the original proposal. Such
modifications include adjusting the OOP cap, adjusting the share of liability
held by each of the stakeholders in the catastrophic phase, and potentially
requiring manufacturers to pay discounts both before and after the catastrophic
phase.
Options for the OOP Cap and How to Index It
Determining where to set the OOP limit is
primarily a question of balancing how many beneficiaries should be protected
from high OOP costs (and the level of protection that should be provided)
against the need for premiums not to increase dramatically, as premiums will
rise as the OOP limit drops, all else being equal. The analysis done by Milliman in July 2018 modelling OOP
maximums between $2,500 and $4,000 illustrates this dynamic. At $4,000, the
cost of the premium increase is expected to be $60.9 billion less over 10 years
relative to what it would be under a $2,500 OOP cap.
For comparison, under the current system
beneficiaries reaching the catastrophic coverage phase in 2020 will spend an
estimated $2,650 in OOP costs before reaching that phase. As a result, setting
the cap at $2,500 provides a comparable threshold to the current system while also
providing financial relief to all beneficiaries reaching catastrophic coverage
(as well as some who are currently just below the threshold). While premiums
are still expected to rise with a $2,500 cap, insurers know the importance of
premiums to beneficiaries when selecting a plan and will likely try to mitigate
increases through various means, including increased utilization management
tools.
Some are also interested in providing a monthly
OOP cap to assist beneficiaries—particularly those individuals on a fixed
income—facing a very high OOP cost in a single month, potentially reaching the
annual OOP cap by January or February. There are two different ways a monthly
OOP cap may be applied, and they would have different impacts. Both methods
have the potential for gaming the system, though, which would consequently
increase insurer liability. As a result, if monthly OOP caps were also
required, premiums would likely increase to some degree beyond what is expected
from simply imposing an annual OOP cap to account for this uncertainty.
A cap that limits OOP expenses in a given month,
such that once the cap is reached the beneficiary will not then nor in the
future be responsible for any more costs incurred that month, could lead to
some manipulating the system. For example, a beneficiary, upon learning that he
will reach the monthly limit, may try to fill all other medications he is
prescribed or multiple doses of a medicine before the month’s end.
Alternatively, a monthly cap could be imposed
that limits OOP spending for a single month but allows any amount over the
monthly cap to still be due in following months, similar to an installment
payment plan. For example, if a beneficiary has an OOP liability of $2,000 one
month, but a $500 monthly cap is imposed, the beneficiary would pay the $2,000
over the course of four months. This method may be less likely to lead to
abuses and lessen the possibility that significant unexpected additional
liabilities will fall to the insurer, which in turn should help keep premiums
from rising. Gaming this structure would still be possible, though, depending
on how the policy deals with a large expense that falls in the final months of
the year. To apply the example from above, if the $2,000 OOP liability occurred
in November, would the beneficiary only have to pay $1,000? If the answer is
yes, then beneficiaries may try to delay treatment regimens until the end of
the year.
An OOP cap, whether annual or monthly, could be
indexed just as the various coverage phase limits are currently: increasing at
the average rate of per capita cost growth in the program.
Share of Catastrophic Liability Held by
Insurers, Manufacturers, and the Government
One feature of AAF’s proposal that has gained
significant attention is that it sets the manufacturer’s liability in the
catastrophic phase at 9 percent. The proposal simply did not intend to take a
position on how much responsibility for the program’s total costs each of the
stakeholders should take, instead respecting the liabilities that Congress has
required to date. Thus, 9 percent was found to be the percentage that would be
budget-neutral for the pharmaceutical industry as a whole over the 10-year
period considered, relative to current projections, based on Milliman’s model
prior to any assumed behavioral changes. That said, AAF’s proposal assumes that
rearranging the liabilities and applying them in the manner suggested more
appropriately aligns incentives and more effectively works to contain program
costs.
Of course, the intent of the proposal is to
change behavior; specifically, it seeks to reduce the prices paid for drugs.
Accordingly, modeling showed the expected impact of AAF’s proposal if it
induced a 5 percent reduction in spending on non-specialty brand-name drugs,
achieved through a combination of price reductions and increased plan
management of high-cost drugs. Analysis by Milliman found that such a change would
reduce the rebates drug manufacturers pay, relative to the baseline scenario,
by $1.6 billion over 10 years.[1] It
is important to note, however, that a reduction in rebates owed does not
necessarily translate to higher revenue for drug companies: Again, those
projected reductions in rebates are based on an assumption that prices and
spending on drugs is reduced. In other words, drug manufacturers would only owe
less in rebates if overall program spending is reduced, essentially allowing
them to share in the savings.
The proposal’s distribution of liability for
plans and the government was largely modeled on the 2016 recommendation
from MedPAC. It seemed appropriate to maintain a
minimum level of government reinsurance of 20 percent, and thus the
manufacturer liability was deducted from the share for which the insurers
otherwise would have been responsible. In April, MedPAC illustrated the trade-offs between
increasing or decreasing the level of liability held by the plans and
manufacturers.[2] Any
change in liability for each of the stakeholders will of course have various
mathematical and behavioral impacts.
Requiring Manufacturer Discounts in the Coverage
Gap and Catastrophic Phase
Some have suggested that manufacturers should
continue paying rebates in the coverage gap in addition to paying rebates in
the catastrophic coverage phase. The impacts of such a change to the proposal
would depend on the rebate amounts required. In order to maintain budget
neutrality for the pharmaceutical industry, as AAF’s original proposal does, it
would necessarily require a lower rebate percentage than 9, likely 5-6 percent,
assuming a flat rate in both phases of coverage. Doing so would certainly
spread the risk more evenly across the pharmaceutical industry but could also
lessen the financial incentive not to increase prices, relative to what a
higher percentage in the catastrophic phase would encourage.
As shown in the second and third columns of the
table below, the current Coverage Gap Discount Program (CGDP) becomes less
impactful as the price of the drug increases because the rebate amount is
indirectly capped. For example, a drug costing $9,303—the lowest price at which
the maximum rebate amount will be required, as explained here—pays a rebate equal to 39.8 percent of
the cost of the drug. A drug priced at $60,000, on the other hand, pays the
same rebate amount, but that amount is equal to only 6.2 percent of the drug’s
price. Thus, the current benefit design is more harmful to lower-priced drugs.
Requiring the rebate in the catastrophic phase of coverage such that it is no
longer capped allows the required rebate amount to increase, both nominally and
as a share of the drug’s price, as the price increases, targeting more of the
burden on the higher-priced drugs. The fourth and fifth columns track the
required rebates under AAF’s proposal for drugs of different prices.
Table 1: Rebates Required Under Various Reform
Proposals
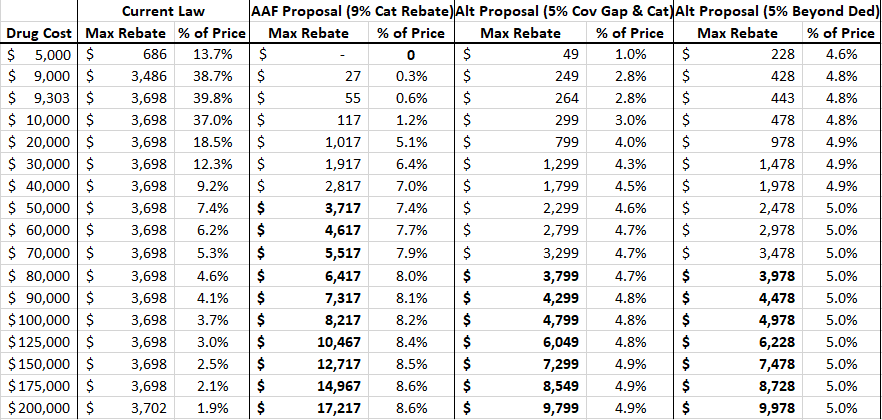
The last four columns of the table show the
rebate amounts under two variations of the AAF proposal: for the sixth and
seventh columns, if rebates were required to be paid in both the coverage gap
and catastrophic coverage phases (in other words, a flat percentage for the
total cost of the drug in excess of the initial coverage limit, which will be
$4,020 in 2020); and in the eighth and ninth columns, a policy that would
require a rebate for any spending above the deductible. As the bolded numbers
indicate, the “break-even price” (at which point the rebate amount required
under these proposals is equal to the rebate amount required under current law)
would be significantly higher than the break-even price for AAF’s original
proposal. Requiring a 5 percent rebate in both the coverage gap and
catastrophic phase would not yield a rebate equal to or greater than $3,698
until the price of the drug reaches $77,980. If a 5 percent rebate were
required for all spending above the deductible, the break-even price would be
$74,395. Prior analysis showed the break-even
price under AAF’s original proposal is $49,784.
Regarding the overall impact, there were 565
drugs for which average spending per beneficiary in 2017 exceeded $4,020 (the
initial coverage limit, or ICL, for a standard benefit plan in 2020), according
to the Centers for Medicare & Medicaid Services’ Drug Spending Dashboard. These drugs were
provided to 3.7 million beneficiaries for a total cost (including spending
before the ICL) of $61.1 billion. To estimate the potential impact of the
policy being considered here, assume spending per beneficiary for all drugs
increases 5 percent from 2017-2020 and utilization for all drugs increases 10
percent (the rate that overall enrollment is expected to increase over this
period). Based on these assumptions, it is estimated that 582 drugs will have
an average cost per beneficiary exceeding the ICL of $4,020 in 2020 and will be
provided to 4.2 million beneficiaries at a total cost of $71.3 billion.
Spending above the ICL for these drugs will equal an estimated $54.3 billion.
If a 5 percent rebate were required from drug manufacturers for all spending in
the coverage gap and catastrophic phase, $2.7 billion in rebates would be
collected on these drugs alone. A 6 percent rebate would provide $3.3 billion
in rebates. Each percentage point increase in rebates required would provide an
additional $543.3 million in rebates. Of course, rebates will also be paid for
drugs costing less than $4,020 if they happen to be prescribed after the
beneficiary has incurred total costs exceeding that amount, but it is difficult
to estimate that impact.
If a rebate were required for any spending that
occurred above the deductible, significantly more drugs would be affected.
Using the same assumptions from the previous analysis, 1,657 drugs will be
provided to 46 million beneficiaries with average spending per beneficiary
exceeding $435 (the deductible for a standard benefit plan in 2020). Total
spending on these drugs, based on the aforementioned assumptions, would equal
$144.9 billion with $124.8 billion occurring after the deductible has been
reached for each of these beneficiaries, assuming they are taking no other
drugs. Requiring a 5 percent rebate for all spending beyond the deductible
would yield $6.2 billion in rebates in 2020 from these drugs. While it remains
true that this total is likely not the entirety of rebates that would be
collected, this does capture a much greater share of overall
rebates that would be collected because spending on these drugs accounts for 82
percent of overall program spending, under these assumptions.
If pharmaceutical discounts are required in any
phase beyond the deductible where the beneficiary would otherwise be expected
to cover a portion of the costs, the share of costs covered by the drug
manufacturers could be used to reduce beneficiary cost-sharing in that phase.
Doing so would allow manufacturer and insurer liability to remain constant
through each of the benefit phases while providing beneficiaries additional
relief. This additional relief would, most notably, benefit patients with lower
annual spending who would not benefit from the imposition of an OOP cap, as
shown below. Alternatively, the manufacturer discounts could be used to reduce
plan liability, which could help offset expected premium increases, reducing
costs for beneficiaries and the direct subsidy paid by the government.
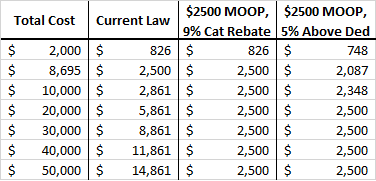
Impact on Beneficiaries with Various Total Drug
Costs
The following table shows the various OOP
requirements that would be required of beneficiaries under various proposals at
various total drug costs. The third column shows the OOP liability under the
original AAF proposal, given various total annual drug costs. Beneficiaries
would pay their deductible plus 25 percent cost-sharing until reaching the
$2,500 OOP cap. The last column shows the OOP liability for the same total
costs under a proposal to require manufacturers to pay 5 percent of costs
incurred after the beneficiary reaches the deductible, reducing beneficiary OOP
liability to 20 percent of costs above the deductible until the $2,500 OOP cap
is reached. As you can see, any beneficiary with total drug spending above
$8,695 will benefit from either of these proposals. The second proposal will
benefit patients with much lower costs.
Table 2: Out-of-Pocket Requirements Under
Various Proposals
Requiring Discounts Only for Non-LIS
Beneficiaries
Some have asked about the rationale in AAF’s
plan to extend the rebate requirement to drugs provided to low-income subsidy
(LIS) beneficiaries, since it currently only applies to non-LIS beneficiaries.
If LIS beneficiaries continued to be excluded from the rebate requirement and
the policy were implemented with the intent of holding the pharmaceutical
industry harmless relative to current law obligations, then the discount rate
currently required in AAF’s proposal would have to be increased. Further, it
has been noted that high-cost LIS beneficiaries use different types of drugs than non-LIS
beneficiaries; thus, the rebates would be more narrowly targeted on specific
drug classes, disproportionately hitting cancer, Multiple Sclerosis, and
rheumatoid arthritis drugs.[3] Depending
on a drug company’s portfolio, such a policy could be particularly harmful or
it could allow for cost-shifting from one product to another, undermining the
intent of the policy. But more uniform policy is less likely to create winners
and losers.
Issues for Further Consideration
Impact of the Rebate Rule
When AAF’s proposal was put forward, the Trump
Administration’s so-called “rebate rule” had not been proposed, and thus it was
not accounted for in any of the modeling done at the time. While AAF has not
yet conducted new modeling, this proposal and the rebate rule are expected, at
least on their own, to have similar effects: slightly higher premiums for
everyone and significant OOP savings for some. If both were to go into effect,
premiums may increase enough to affect enrollment. Policymakers should carefully
consider the combined effect before moving forward with both proposals.
If the rebate rule were implemented before this
structural reform, it is almost certain that a lower OOP cap would be required
to keep the overall spending that occurs before catastrophic coverage at
roughly the same level, which in turn would keep expected manufacturer rebates
at roughly the same level. Otherwise, less spending would occur in the
catastrophic phase and manufacturers would be liable for less of the costs.
There would, however, be no impact on beneficiary OOP spending if the OOP cap
were kept at the same level.
It may also be true, however, that the
structural changes proposed here—specifically, the OOP cap—may largely mitigate
the need for or impact of the rebate rule. Both policies seek to reduce the OOP
burden of high-cost drugs. And, more specifically, the rule has the largest
impact on the OOP costs for drugs with coinsurance. To the extent that
these drugs push a beneficiary into the catastrophic phase, the full value of
the OOP reduction that would result from the rebate rule may exceed the
beneficiary’s OOP liability under our proposal. In such an instance, the rebate
may again be used for premium reduction. Thus, estimating the impact of the
policies implemented in tandem is not likely as simple as adding the expected
impact of each individually.
Effect of Price Increases by Manufacturers
Indeed, drug manufacturers may simply increase
the prices of their drugs by the amount of the rebate they will be required to
pay. In fact, prior work by AAF has argued that this
phenomenon is likely already occurring as a result of the current CGDP, as well
as the Medicaid Drug Rebate Program, the 340B Drug Discount Program, and the taxes
imposed on pharmaceutical sales after passage of the Affordable Care Act.
Mandatory discounts and taxes distort the market and increase prices, which is
why this proposal is not a policy that would be beneficial apart from the
current set of policies. That said, this proposal is less likely to encourage
price inflation than the current structure because of the fact that the rebates
increase along with the price of the drug, as explained earlier. In other
words, there is less pay-off for a price increase under this proposal than
under current law, which is the primary rationale for making this change.
Current Structure May be Discouraging Use of
Lower-Cost Generics
The current benefit structure may also encourage
use of higher-priced drugs as a result of the differences in insurer liability
between brand-name and generic drugs. Insurers are currently responsible for
just 5 percent of the cost of a brand-name or biosimilar drug in the coverage
gap but 75 percent of the cost of a generic drug. Therefore, unless a
brand-name drug costs more than 15 times more than the generic, the insurer
will pay less for the brand-name drug in the coverage gap. Further, plans have
no liability for LIS enrollees in the coverage gap, which MedPAC suggests may
explain why LIS beneficiaries have lower generic utilization rates than
non-LIS.[4]
Conclusion
In the 16 years since Congress created the
Medicare Part D program, the prescription drug market, insurance structure,
and pricing practices have changed. Patterns
have emerged that make it clear the current system is encouraging undesirable behaviors that increase costs
for the government and consumers. Reforming the benefit structure in a way that
realigns the financial incentives of both the insurers and drug manufacturers
may help to reverse these trends by putting downward pressure on drug prices.
Such a substantial reform requires careful consideration of the many trade-offs
that will result from those changes.
[1] http://us.milliman.com/insight/2018/Restructuring-the-Medicare-Part-D-benefit-with-capped-beneficiary-spending/
[2] http://www.medpac.gov/docs/default-source/default-document-library/options-to-increase-the-affordability-of-specialty-drugs-in-pt-d—final.pdf?sfvrsn=0 (Slide
12)
[3] http://medpac.gov/docs/default-source/reports/jun19_ch2_medpac_reporttocongress_sec.pdf?sfvrsn=0 (page
44)
[4] http://www.medpac.gov/docs/default-source/reports/jun19_ch2_medpac_reporttocongress_sec.pdf?sfvrsn=0 (page
42)
https://www.americanactionforum.org/insight/what-congress-needs-to-consider-when-reforming-medicare-part-d/#ixzz5serjHGbq
Follow @AAF on Twitter
No comments:
Post a Comment