Gretchen Jacobson Follow @GretchJacob on
Twitter, Tricia Neuman Follow @tricia_neuman on
Twitter, and Anthony Damico Published:
May 07, 2019
Overview
Medicare payments to Medicare HMOs and PPOs,
known as Medicare Advantage plans, have always been based on Medicare spending
by similar people in traditional Medicare, partly because Medicare has never
had accurate, complete data on the use of services or health care spending for
beneficiaries in Medicare Advantage plans.1 The assumption has been that adjusting
payments to plans for health status and other factors accounts for differences
between beneficiaries in traditional Medicare and those in Medicare Advantage
plans. Profits are assumed to be due to plans reducing spending by either
managing fees (e.g., by having lower-cost hospitals in their network) or
changing patterns of care (e.g., reducing hospital readmissions), rather than
to favorable selection. Nonetheless, selection bias has been an ongoing concern
and the subject of many studies over the years, with mixed evidence of
favorable selection.2,3,4,5,6 This question is important because it
affects the accuracy of Medicare payments to plans on behalf of 20 million
Medicare beneficiaries, and rising.
This is the first known analysis to examine
whether beneficiaries who choose to enroll in Medicare Advantage plans have
lower spending and use fewer services – before enrolling in Medicare Advantage
– than similar people in traditional Medicare. If Medicare Advantage enrollees
use fewer services and have lower Medicare spending before they enroll in
Medicare Advantage plans, compared to similar beneficiaries in traditional
Medicare, then basing payments to Medicare Advantage plans on the Medicare
spending for similar beneficiaries in traditional Medicare would overestimate
the expected costs of Medicare Advantage enrollees and overpay plans by
billions of dollars over the next decade. Studies that have looked at
differences in the use of services and Medicare spending for Medicare Advantage
enrollees compared to beneficiaries in traditional Medicare that did not
account for actual prior differences may have overestimated the extent to which
plans are reducing enrollees’ spending or use of services.
To address this question, we examine Medicare
Part A and B spending and service use for traditional Medicare beneficiaries in
2015. We compare average Medicare spending and use of services for traditional
Medicare beneficiaries who enrolled in Medicare Advantage plans versus those
who remained in traditional Medicare in 2016, after adjusting spending values
for health conditions and other relevant factors (Figure 1). We examine how the
results differ across demographics, chronic conditions, and counties, and also
examine how the results change when Part D spending is included. The analysis
is based on a five percent sample of Medicare claims data and excludes
beneficiaries who may not have been active choosers in 2016; more details about
the analysis are included in the Methods.
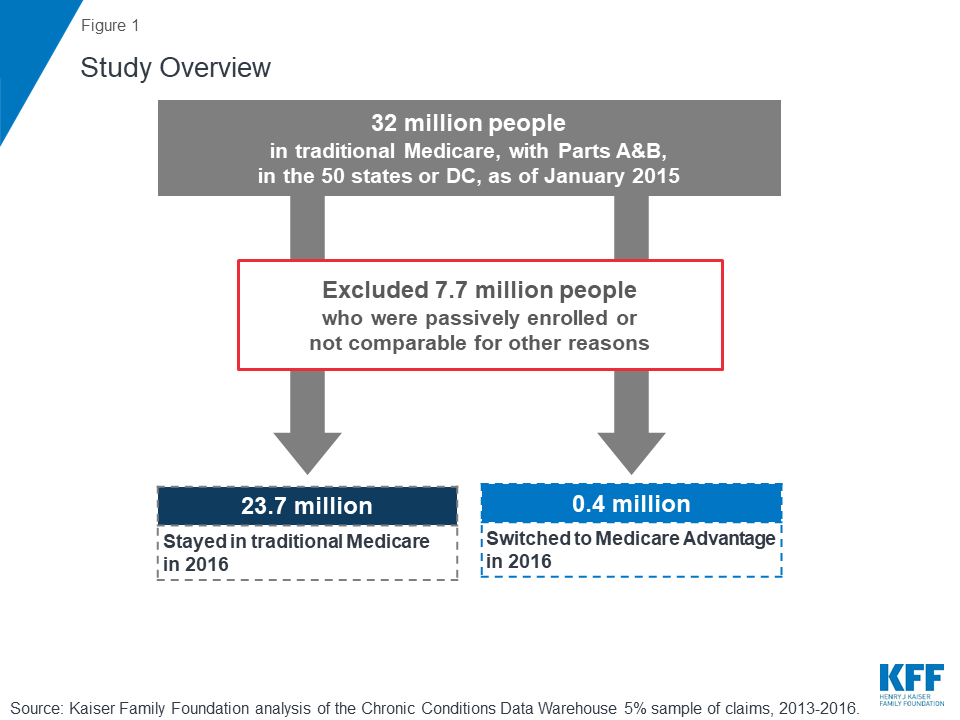
Figure 1: Study
Overview
Differences in
Medicare Spending
Among beneficiaries in traditional Medicare in
2015, those who enrolled in Medicare Advantage in 2016 had spending (for Part A
and Part B) that was $1,253 lower (13% difference), on average, than
beneficiaries who remained in traditional Medicare in 2016, after adjusting for
health risk factors (Figure 2; Tables 1 and
2).7
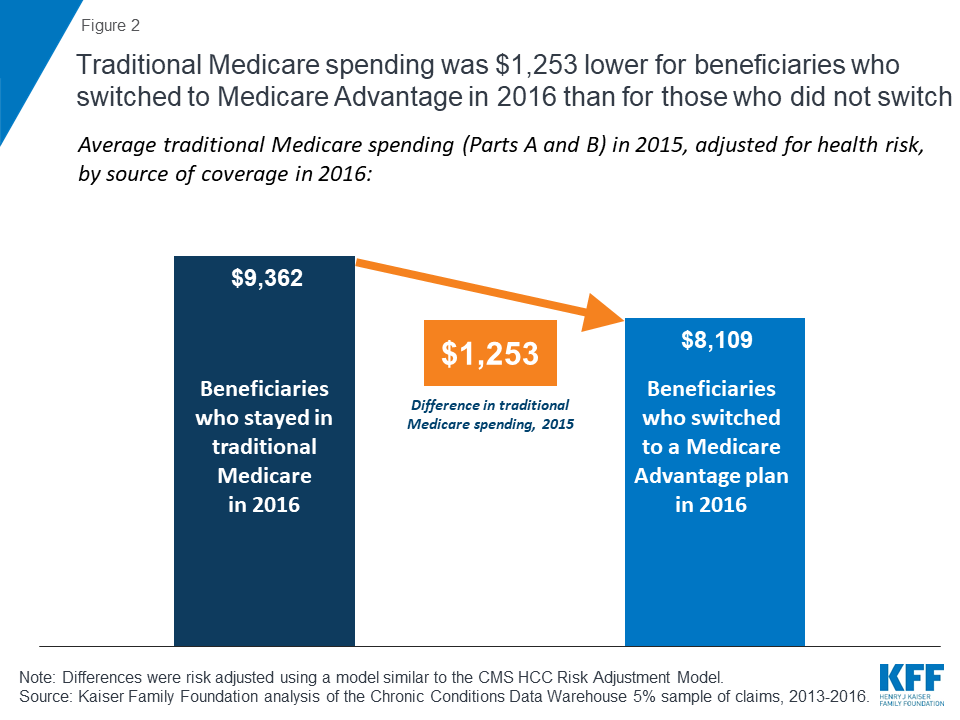
Figure 2: Traditional
Medicare spending was $1,253 lower for beneficiaries who switched to Medicare
Advantage in 2016 than for those who did not switch
When Part D spending is included, the results
changed only slightly. Traditional Medicare beneficiaries in 2015 who switched
to Medicare Advantage in 2016 had total Medicare spending (including Part D)
that was 15 percent lower than spending for beneficiaries who remained in
traditional Medicare in 2016.
Comparison to Other Payments
Received by Medicare Advantage Plans. To put the difference in Medicare spending in context, the
$1,253 average difference in spending is nearly four-times larger than the
average per capita quality-based bonus payment ($336) paid to Medicare
Advantage prescription drugs plans that qualified for bonuses in 2015 (Figure
3). The average difference in spending is also more than twice as large as the
average annual premium paid by Medicare Advantage enrollees in 2015, including
enrollees in plans with no premium.
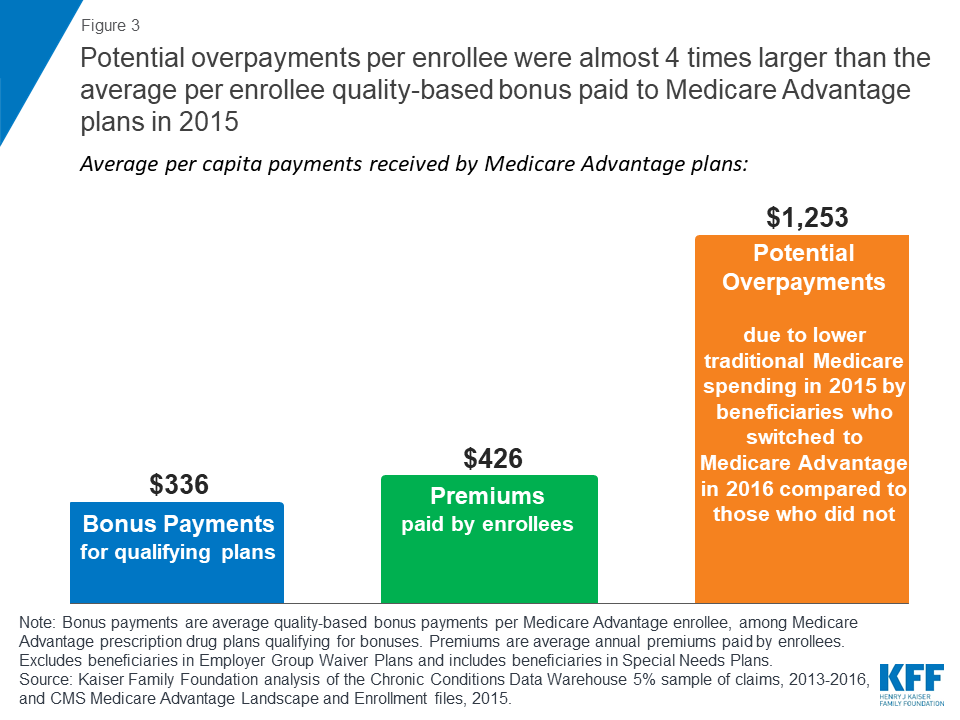
Figure 3: Potential
overpayments per enrollee were almost 4 times larger than the average per
enrollee quality-based bonus paid to Medicare Advantage plans in 2015
Differences in
Medicare Spending, by Demographics
Traditional Medicare spending in 2015 was
lower for beneficiaries who enrolled in Medicare Advantage plans in 2016 than
for similar beneficiaries who remained in traditional Medicare that year, by
age and gender, and among beneficiaries dually eligible for Medicare and
Medicaid, after adjusting for health risk and other factors (Table 1).
·
Age: The difference
in average traditional Medicare spending in 2015 among beneficiaries who
switched to Medicare Advantage in 2016, compared to those who remained in
traditional Medicare, was evident for beneficiaries of all ages, and increased
with age for beneficiaries over the age of 65, after risk adjustment. For
example, among beneficiaries ages 65-69, average traditional Medicare spending
in 2015 was $1,119 lower among beneficiaries who switched to a Medicare
Advantage plan in 2016 than for similar beneficiaries who remained in
traditional Medicare; among beneficiaries ages 85-89, the difference in
spending was $1,314. This finding suggests that selection bias, and the
associated potential overpayments, may increase with age.
·
Gender: The average
difference in spending between the two groups was similar among men and women
($1,271 and $1,247, respectively).
·
Dual eligibility for Medicaid: Traditional Medicare spending in 2015 for Medicare
beneficiaries with full Medicaid benefits (full dual eligible) who enrolled in
Medicare Advantage in 2016 was $1,142 lower, on average, than spending for
similar full dual eligibles who stayed in traditional Medicare in 2016, after
adjusting for health and demographic factors. Similarly, partial dual eligibles
who enrolled in Medicare Advantage in 2016 had traditional Medicare spending in
2015 that was $1,162 lower than spending for those who remained in traditional
Medicare in 2016, after adjusting for risk factors. In other words, among
dually eligible beneficiaries – a group of beneficiaries with relatively high
Medicare spending – those who used more services and incurred higher Medicare
spending in 2015 were more likely to remain in traditional Medicare in 2016
while dual eligibles with lower service use and spending were more likely to
enroll in a Medicare Advantage plan in 2016.
·
Institutional status: Among Medicare beneficiaries living in institutions, such as
nursing homes, traditional Medicare spending in 2015 was $1,825 lower among
those who enrolled in Medicare Advantage plans in 2016 than among similar
institutional residents who stayed in traditional Medicare that year. If
higher-cost nursing home residents are remaining in traditional Medicare while
lower-cost residents are moving to Medicare Advantage plans, it could make it
easier for Medicare Advantage plans serving the nursing home population to be
profitable, which may explain the relatively recent increase in firms offering
Special Needs Plans for this population (I-SNPs).8
Differences in
Medicare Spending, by Chronic Conditions
Even among beneficiaries with the same chronic
conditions, those who enrolled in Medicare Advantage plans in 2016 consistently
had lower Medicare spending in 2015 than similar beneficiaries who remained in
traditional Medicare in 2016 (Table 1).
For example, among traditional Medicare
beneficiaries with diabetes in 2015, those who enrolled in Medicare Advantage
plans in 2016 had Medicare spending that was $1,072 lower in 2015, on average,
than similar beneficiaries with diabetes who stayed in traditional Medicare in
2016, after adjusting for differences in health status (Figure 4). In other
words, it would appear that lower-cost beneficiaries with diabetes are more
inclined to enroll in Medicare Advantage than higher-cost diabetics. Likewise,
traditional Medicare beneficiaries with asthma who enrolled in Medicare
Advantage plans in 2016 had Medicare spending that was $1,410 lower in 2015, on
average, than similar beneficiaries with asthma who remained in traditional
Medicare in 2016, even after adjusting for health risk factors.
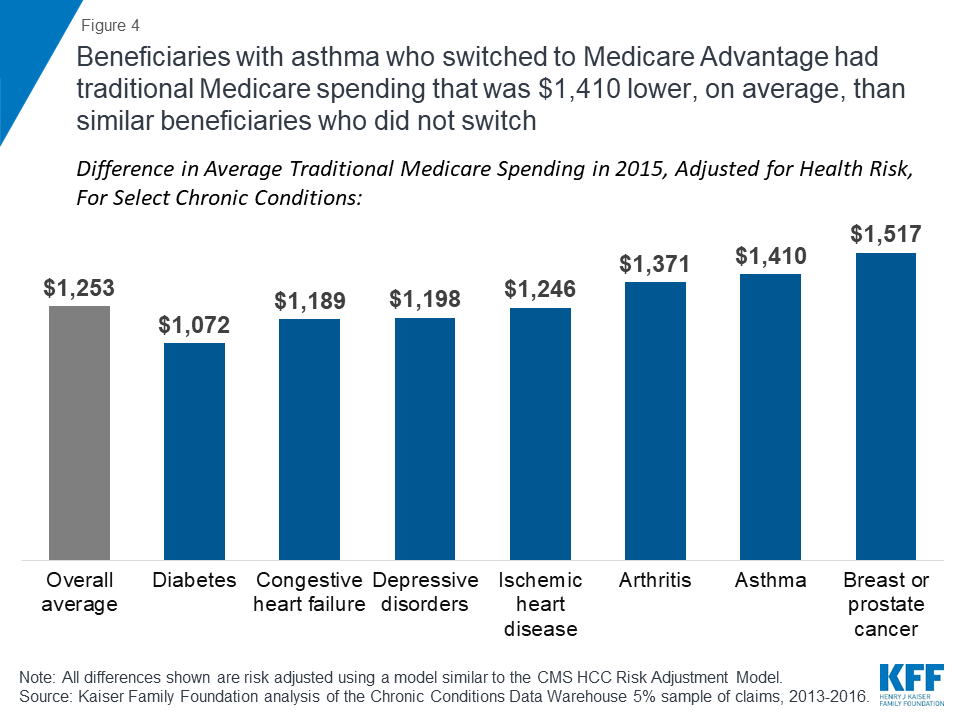
Figure 4:
Beneficiaries with asthma who switched to Medicare Advantage had traditional
Medicare spending that was $1,410 lower, on average, than similar beneficiaries
who did not switch
The difference in average, adjusted 2015
traditional Medicare spending between beneficiaries who subsequently enrolled
in Medicare Advantage versus those who remained in traditional Medicare
increases with the number of chronic conditions, rising from $226 among those
with no chronic conditions to $1,629 or more among beneficiaries with 5 or more
chronic conditions (Figure 5). This finding suggests that potential
overpayments may be largest for the Medicare Advantage plans that are serving
the sickest beneficiaries.
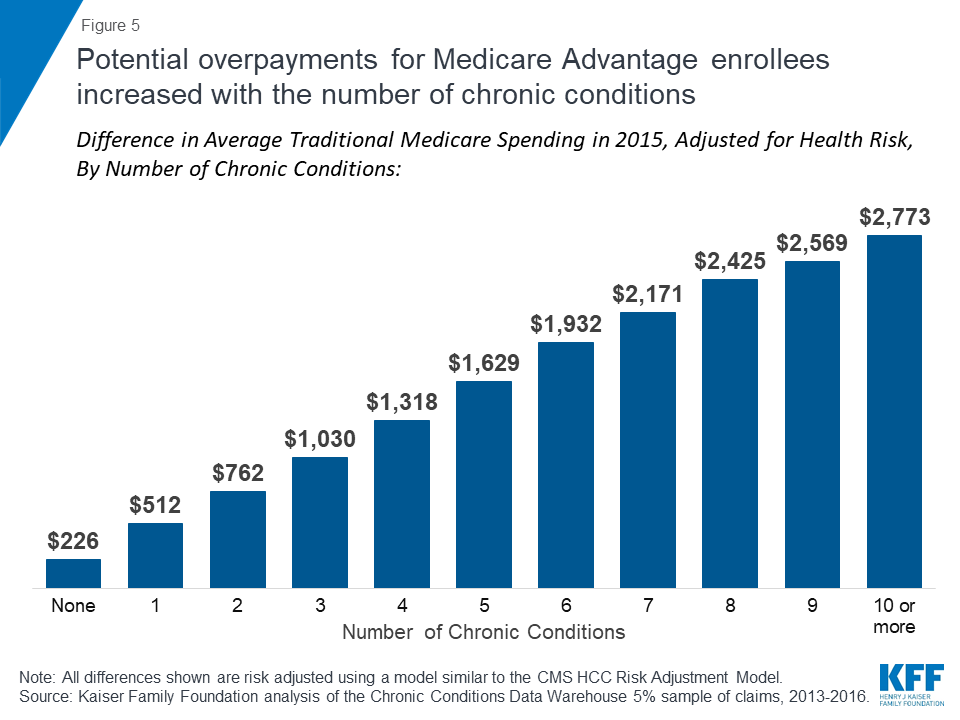
Figure 5: Potential
overpayments for Medicare Advantage enrollees increased with the number of
chronic conditions
Differences in
Medicare Spending, by County
In this section, we looked at whether the
observed differences in spending and service use persist across markets, and
the extent to which differences may vary from one market to another. We
compared average spending in 2015 among beneficiaries who switched to Medicare
Advantage in 2016 versus those who remained in traditional Medicare, without
adjusting for other factors. We were not able to replicate the analysis by
county with the adjustment for risk factors, such as health conditions and
demographics, due to sample size constraints. For this analysis, we looked at
20 relatively large markets that vary geographically, and vary by Medicare
Advantage penetration and payment quartiles.
Among large, urban counties, the differences
in spending between Medicare Advantage enrollees and beneficiaries in
traditional Medicare varied greatly across the country (Figure 6; Table 3). In
some counties, such as Los Angeles, CA, San Bernardino, CA, Wayne, MI
(Detroit), and Cuyahoga, OH (Cleveland), beneficiaries who enrolled in Medicare
Advantage plans in 2016 had significantly lower traditional Medicare spending
in 2015 ( ≥$3,000 lower) than beneficiaries in the county who remained in
traditional Medicare in 2016.
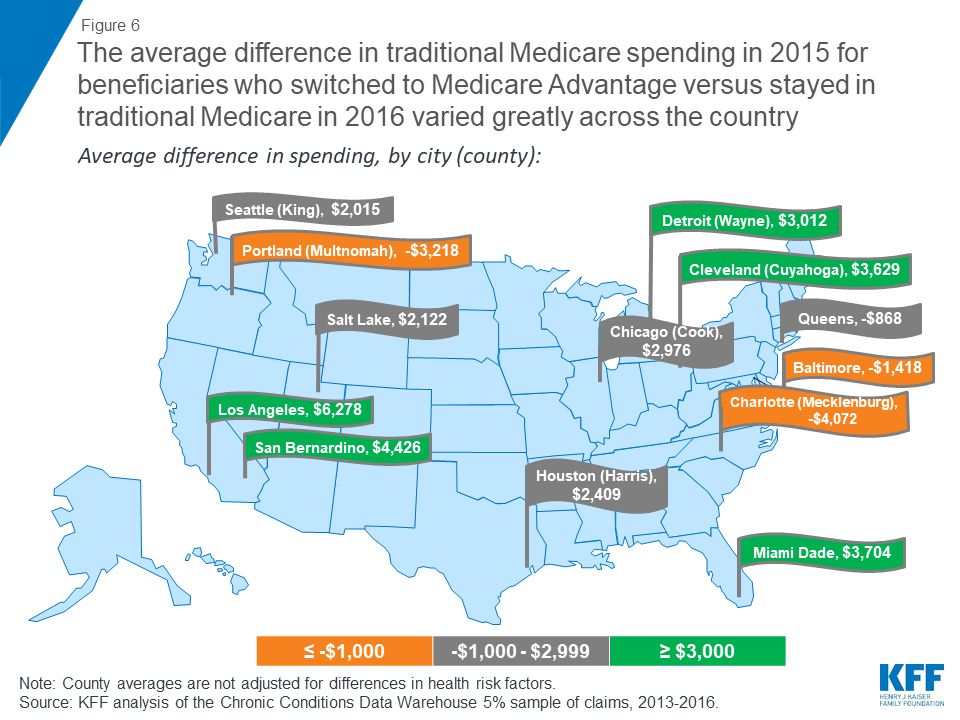
Figure 6: The average
difference in traditional Medicare spending in 2015 for beneficiaries who
switched to Medicare Advantage versus stayed in traditional Medicare in 2016
varied greatly across the country
In other counties, such as Allegheny, PA
(Pittsburgh), Baltimore City, MD, Mecklenburg, NC (Charlotte), Erie, NY
(Buffalo), and Multnomah, OR (Portland) beneficiaries who enrolled in Medicare
Advantage plans in 2016 had higher prior year traditional Medicare spending (
≤-$1,000) than beneficiaries in the county who remained in traditional Medicare
in 2016. These differences across counties suggest that the selection bias into
Medicare Advantage may vary across markets.
Discussion
This analysis examines whether beneficiaries
who choose to enroll in Medicare Advantage plans have lower spending and use
fewer services – before enrolling in Medicare Advantage – than similar people
in traditional Medicare. The study found that beneficiaries who chose to enroll
in a Medicare Advantage plan in 2016 had average expenditures in traditional
Medicare (in 2015) that were $1,253 less, on average, than similar
beneficiaries who remained in traditional Medicare. Similar differences in
spending were found across all demographics and chronic conditions, even after
adjusting for health risk factors. The results suggest that favorable
self-selection into Medicare Advantage plans is occurring, even among
traditional Medicare beneficiaries with similar health conditions. The findings
raise questions as to why beneficiaries who are higher utilizers are less
likely to go into Medicare Advantage and instead remain in traditional
Medicare.
Other studies have examined services used by
people while they were enrolled in Medicare Advantage plans, based on limited
data, and have generally found that beneficiaries in Medicare Advantage plans
use fewer services than those in traditional Medicare.9,10,11 Notably, the authors of these studies
almost universally attribute differences in service utilization to care
management by the plans – rather than to pre-existing differences in care seeking
behavior and use of health services. This study suggests that differences in
health care use, and spending, are evident before beneficiaries decided to
enroll in Medicare Advantage plans or remain in traditional Medicare, raising
questions about the extent to which plans are actually lowering spending or
managing care.
It is not clear whether the differences in
spending observed in this study increase, decrease, or persist over time as
beneficiaries age, which has implications for whether a similar difference in
spending could be assumed for all Medicare Advantage enrollees.12 Likewise, it is not clear how this
difference in spending will change as the share of counties with the majority
of beneficiaries in Medicare Advantage plans grows. This missing information
could have important implications for Medicare spending. Potential overpayments
could amount to billions in excess Medicare spending over a ten-year period if
the observed differences in spending hold up as beneficiaries age and Medicare Advantage
enrollment continues to rise. To illustrate, if the difference in average
Medicare spending ($1,253) applied to just 10 percent of all Medicare Advantage
enrollees in 2016, or 1.8 million enrollees, it would amount to more than $2
billion in excess spending in one year alone.
Policymakers could consider adjusting payments
to reflect Medicare Advantage enrollees’ prior use of health care services,
which could lower total Medicare spending and in turn reduce Medicare Part B
premiums and deductibles for all beneficiaries. With more than 20 million
enrollees in Medicare Advantage plans and Medicare payments to plans projected
to reach $250 billion in 2019, the stakes are high for making payments to plans
as accurate as possible.13,14
Gretchen Jacobson and
Tricia Neuman are with the Kaiser Family Foundation. Anthony Damico is an
independent consultant.
This paper benefitted
from the methodological expertise of Bianca Frogner at the University of
Washington.
https://www.kff.org/report-section/do-people-who-sign-up-for-medicare-advantage-plans-have-lower-medicare-spending-issue-brief/
No comments:
Post a Comment