Rachel
Dolan Published: Nov 12, 2019
Drug
prices are at the center of health policy debates at both the state and federal
levels. Medicaid provides health coverage for millions of Americans, including
many with substantial health needs. Prescription drug coverage is a key
component of Medicaid for many beneficiaries who rely on medications for both
acute problems and for managing ongoing chronic or disabling conditions.
Without Medicaid, many prescription drugs would be prohibitively expensive to
low-income beneficiaries. Both state and federal policymakers are
undertaking efforts to control prescription drug costs, and there is renewed
policy interest in the Medicaid Prescription Drug Rebate Program (MDRP) as part
of these efforts. Policymakers are also currently debating significant changes
to payment for prescription drugs through Medicare and commercial insurers that
may also have implications for Medicaid and the MDRP as well. This brief
explains the MDRP to help policymakers and others understand how Medicaid pays
for drugs and any potential consequences of policy changes for the program by
answering the following questions:
- What is the MDRP
and how does it work?
- What is the
impact of the MDRP?
- What is the role
of managed care plans and pharmacy benefit managers in Medicaid rebates?
- How does the
340B program interact with the MDRP?
- What are policy
proposals related to the MDRP?
What is
the Medicaid drug rebate program and how does it work?
In response to rising
drug prices and projected increased Medicaid spending, the Medicaid
Prescription Drug Rebate Program (MDRP) was created in 1990 by the Omnibus
Reconciliation Act.1,2
Under the program, a manufacturer who wants its drug covered under Medicaid
must enter into a rebate agreement with the Secretary of Health and Human
Services stating that it will rebate a specified portion of the Medicaid
payment for the drug to the states, who in turn share the rebates with the
federal government. Manufacturers must also enter into agreements with other
federal programs that serve vulnerable populations. In exchange, Medicaid
programs cover nearly all of the manufacturer’s FDA-approved drugs, and the
drugs are eligible for federal matching funds. Though the pharmacy
benefit is a state option, all states cover it, but, within federal guidelines
about pricing and rebates, administer pharmacy benefits in somewhat different
ways.
The MDRP affects state
and federal Medicaid payment for prescription drugs, while Medicaid
beneficiaries’ out of pocket cost for drugs is limited to nominal amounts set
in statute. Due to Medicaid’s role in financing coverage for high-need
populations with low incomes, it is designed to provide access to prescription
drugs with little cost to enrollees. Federal rules limit beneficiary
cost-sharing to nominal amounts: up to $4 for preferred drugs and $8 for
non-preferred drugs, for individuals with incomes at or below 150% of the
federal poverty level (FPL) and slightly higher for those with higher incomes.3 Not
all states impose cost-sharing for prescription drugs,4 and
some beneficiary groups are exempt from cost-sharing requirements.
The Affordable Care Act
(ACA) made significant changes to the prescription drug rebate program. The law increased the
rebate amount for both brand drugs and generic drugs. It also extended rebates
to outpatient drugs purchased for beneficiaries covered by Medicaid managed
care organizations (MCOs).5 Previously only
drugs purchased through Medicaid fee-for-service were eligible for rebates even
though most states contract with MCOs to provide services to Medicaid
beneficiaries.6
The Medicaid rebate
amount is set in statute and ensures that the program gets the lowest price
(with some exceptions).7 The
formula for rebates varies by type of drug: brand8 or
generic. The rebate formula is the same regardless of whether states pay for
drugs on a fee-for-service basis or through payments to managed care plans. The
specific rebate on a given drug is considered proprietary. For brand name
drugs, the rebate is 23.1% of Average Manufacturer Price (AMP) or the
difference between AMP and “best price,” whichever is greater. Certain
pediatric and clotting drugs have a lower rebate amount of 17.1% (Figure 1).
Best price is defined as the lowest available price to any wholesaler,
retailer, or provider, excluding certain government programs, such as the
health program for veterans.9 AMP is defined as the average price paid
to drug manufacturers by wholesalers and retail pharmacies.10,11
For generic drugs, the rebate amount is 13% of AMP, and there is no best price
provision.
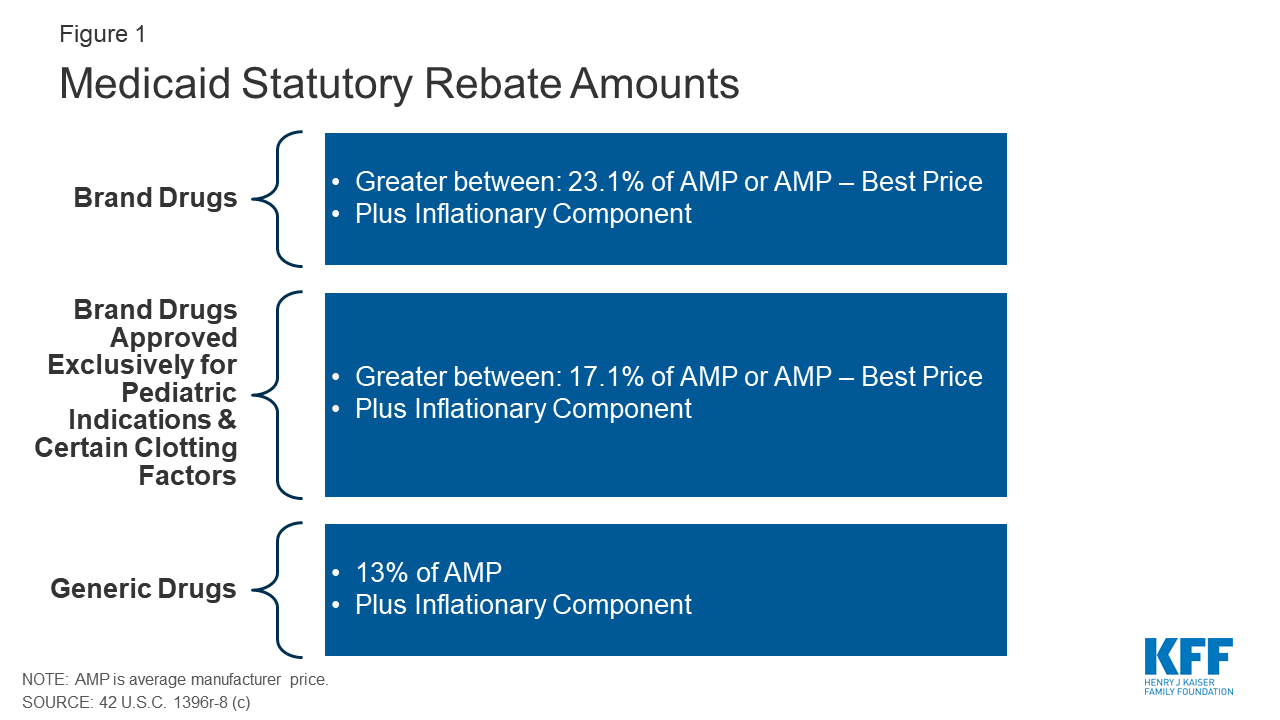
Figure 1: Medicaid
Statutory Rebate Amounts
The rebate calculation
also includes an additional inflationary component to account for rising drug
prices over time. This rebate is calculated as the difference between the drug’s
current quarter AMP and its baseline AMP adjusted to the current period by the
Consumer Price Index for All Urban Consumers (CPI-U).12 In
other words, if a drug’s price increases faster than inflation, the
manufacturer has to rebate the difference to Medicaid. The inflationary
component is an increasing share of brand drug rebates, accounting for more
than half of the total brand drug rebate amounts in 2012.13
Because of the inflationary component, the calculated rebate on a drug whose
price increases quickly over time could be greater than the AMP for that drug.
However, the total rebate amount currently is capped at 100% of AMP.14
In addition to federal
statutory rebates, most states negotiate with manufacturers for supplemental
rebates. As of June 2019, 47 states and DC had supplemental rebate
agreements in place.15
These supplemental rebates are not subject to the best price floor. States
often use placement on a preferred drug list (PDL) as leverage to negotiate
supplemental rebates with manufacturers. States encourage providers to
prescribe drugs on the PDL over other drugs and create incentives for them to
do so if possible. For example, a state may require a prior authorization for a
drug not on a preferred drug list. Often, drugs on PDLs are cheaper or include
drugs for which a manufacturer has provided supplemental rebates. A few states
have used their supplemental rebate authority to negotiate alternative payment
models with manufacturers. States have also formed multi-state purchasing pools
when negotiating supplemental Medicaid rebates to increase their negotiating
power. More than half of states participate in a multi-state supplemental
rebate pool.16 In
addition, Medicaid managed care plans may negotiate their own supplemental
rebate agreements with manufacturers.
Both states and the
federal government play a role in administering the MDRP. Manufacturers must report
AMP for all covered outpatient drugs to HHS and report their best price for
brand name drugs. HHS uses this price data to calculate the unit rebate amount
(URA) based on the rebate formula and inflationary component and provides the
URA to states.17 States multiply the
units of each drug purchased by the URA and invoice the manufacturer for that
amount. Manufacturers then pay states the statutory rebate amount as well as
any negotiated supplemental rebates.
Prescription drug rebates
are shared between the federal and state governments. States and the federal
government share in the statutory rebate amount based on the federal medical
assistance percentages (FMAP), which is the share of Medicaid spending in each
state paid for by the federal government. Manufacturers submit rebates directly
to states.18
The ACA increased rebate amounts from 18.1% to 23.1% for brand drugs and from
11% to 13% for generics, but the state share is only calculated off the pre-ACA
rebate amount, which means the federal government now gets a bigger share of
the rebates.19
What is
the role of managed care plans and pharmacy benefit managers in Medicaid
rebates?
As more states have
enrolled additional Medicaid populations into managed care arrangements over
time, managed care organizations (MCOs) have played an increasingly significant
role in administering the Medicaid pharmacy benefit. More than two-thirds of
Medicaid beneficiaries received their coverage through MCOs in 2017.20 States
pay MCOs a monthly fee (capitation rate) to cover the cost of services provided
to enrollees and any administrative expenses. States may include all Medicaid
services in these contracts or they may “carve-out” certain services, like
prescription drugs, from capitation rates. Managed care plans whose contracts
include coverage for prescription drugs are allowed to negotiate their own
rebates with manufacturers. As with supplemental rebates negotiated by states,
additional rebates for managed care plans can be used to determine placement on
the PDL.
The ACA extended federal
statutory rebates to prescription drugs provided under Medicaid managed care
arrangements, and most states now “carve in” prescription drugs. Prior to the ACA,
manufacturers only had to pay rebates for outpatient drugs purchased on a
fee-for-service basis, not those purchased through managed care. This
encouraged states to “carve out” prescription drugs so they would be able to
get rebates. Extending rebates to drugs purchased through managed care has
resulted in more states carving drug coverage back into managed care. Of the 40
states contracting with comprehensive risk-based MCOs in 2018, 35 states
reported that the pharmacy benefit was carved in, with some states reporting
exceptions such as high-cost or specialty drugs.21
Many states also use
pharmacy benefit managers (PBMs) in their Medicaid prescription drug programs. PBMs perform
financial and clinical services for the program, administering rebates,
monitoring utilization, and overseeing preferred drug lists.22 PBMs
may be used regardless of whether the state administers the benefit through
managed care or on a fee-for-service basis. Some states are reassessing their
use of PBMs in managed care due to issues with the lack of transparency around
PBM payments and the prevalence of “spread pricing.” Spread pricing refers to
the difference between the payment the PBM receives from the MCO and the
reimbursement amount it pays to the pharmacy.23 In
the past, PBMs have been able to keep this “spread” as profit, but a number of
states are implementing policies to curb or altogether prohibit this practice.24
How
does the 340B program interact with the MDRP?
The Medicaid rebate
program interacts with other programs that receive manufacturer discounts on
drugs. As a condition of participation in the Medicaid Drug Rebate program,
manufacturers must also participate in the federal 340B program. The 340B
program offers discounted drugs to certain safety net providers that serve
vulnerable or underserved populations, including Medicaid beneficiaries.25
340B ceiling prices are calculated to match Medicaid prices net of the rebate,
but manufacturers can provide additional discounts to 340B providers that are
not subject to the best price rule.26
Because the 340B program
is administered separately, as stipulated by federal law, states and safety net
providers must ensure that manufacturers do not pay duplicative discounts for
Medicaid beneficiaries.27 Safety net providers
eligible for 340B discounts can choose whether or not they provide drugs
purchased with the program discounts to Medicaid beneficiaries within state
guidelines.28,29 States
may require providers to make the same decision for FFS and managed care
enrollees to streamline the process of determining which claims are eligible
for rebates. To avoid charging manufacturers a duplicate discount, state
Medicaid programs reference a list of safety net providers that provided drugs
under 340B to Medicaid beneficiaries, and the Medicaid program will exclude
their drug claims from their invoices to manufacturers.30
The file does not include drugs paid for by managed care plans or those
dispensed at contract pharmacies, but MCOs also are required to exclude 340B
claims from reports they provide to states for rebate purposes.31,32
There are concerns the list can be out of date or inaccurate, so some states
maintain their own lists or use claims data to avoid duplicate discounts.
Although Medicaid best price and 340B ceiling prices are closely related, the
rules states set for how they reimburse pharmacies may have implications for
drug costs.33,34
What is
the impact of the MDRP?
The rebate program
offsets Medicaid costs and reduces federal and state spending on drugs. In 2017, Medicaid spent
$64 billion on drugs and received nearly $35 billion in rebates. Net spending
on outpatient drugs comprises 5% of total Medicaid benefits spending. While
gross prescription drug spending has increased substantially over time (from
$43 billion in 2014 to $64 billion in 2017) rebates have held net spending
growth to a much lower rate (Figure 2). Gross spending on drugs increased 48%
from 2014-2017, while net spending only increased 25% over the same time
period. Net spending actually declined from 2016-2017.35 In
comparison to other programs, like Medicare Part D, rebates in Medicaid are a
much larger share of drug spending. Medicare actuaries predicted Medicare Part
D rebates to reach 23% of drug spending in 2017 and 25% in 2018.36 In
contrast, Medicaid rebates accounted for 55% of drug spending in 2017.
Figure 2: Medicaid Drug
Spending and Rebates, FY2014-17
The structure of the
rebate program essentially creates an open formulary. When a manufacturer
enters into a rebate agreement with HHS, Medicaid agrees to cover nearly all
FDA-approved drugs from that manufacturer. This approach is different from
private insurers who can enter into negotiations with manufacturers about
whether or not drugs will be on their formularies, leveraging rebates for drugs
that are included or covered with lower patient cost-sharing. While the Medicaid
rebate structure enables beneficiaries to access a wide range of drugs, it also
places some limits on states’ ability to negotiate with manufacturers. This
challenge is particularly acute for new, blockbuster drugs that Medicaid
programs must cover with little leverage to negotiate lower costs.
Medicaid prices and the
rebate program may have implications for prices paid by other payers. There has been increased
attention by policymakers and the public to high list prices, with some brand
name drugs launching with price tags of hundreds of thousands of dollars or
more. Amidst the discussion of high launch prices, analyses of potential
solutions have highlighted the role of the MDRP in the larger drug pricing
system. Some have suggested that the “best price” provision and the rebate
requirements inflate launch prices to account for the rebate and reduce rebates
for other payers (like private insurers) to avoid triggering the best price
provision. Medicare Part D rebates are not included in the best price
calculation. An analysis from CBO was conducted in 1996, shortly after the
creation of the Rebate Program, and showed some initial price increases but
found increases due to MDRP ceased within a few years.37 In
analyzing the potential impact of the ACA rebate provisions, which increased
the rebate amount, CBO estimated a small impact on launch prices.38
What
are policy debates and proposals about the MDRP?
There is renewed policy
interest in the MDRP as states and the federal government explore policies
related to drug costs. Proposals at both the state and federal level would make
changes directly to the MDRP, and proposed changes to other programs may have
implications for Medicaid as well.
Increasing
the Effective Rebate Amount in the MDRP
Because the MDRP is a
complex program that has evolved over time, it contains some technical issues
and provisions that lower the rebate amount paid for some drugs. Policymakers
are considering several changes to address these issues and increase the
effective rebate amount. While these changes would produce savings for both the
federal and state government, authority for undertaking them rests at the
federal level, since the MDRP is in federal statute.
One proposed approach is
to lift the cap on rebates, which is currently 100% of AMP. Because of rising
prices over time, a number of drugs have reached the rebate cap. Increasing or
eliminating the cap would generate savings for the program and lower revenues
for drug manufacturers.39 The
Medicaid and CHIP Payment and Advisory Commission (MACPAC) recommended
eliminating the cap entirely.40 A
bipartisan bill addressing drug costs passed out of the Senate Finance
Committee includes a provision to increase the cap to 125% of AMP.
Another policy proposal
to increase the Medicaid rebate amount is to change the rebate calculation.
Some manufacturers have reduced their rebate obligations by blending the price
of an authorized generic with a brand name drug, which reduces the AMP of the
brand drug. This occurs when a brand drug manufacturer also produces the
authorized generic and the price of both drugs is included in the brand drug’s
AMP. Because the rebate calculation is based on AMP, an artificially low
AMP reduces the rebate a manufacturer pays. Legislation enacted in Fall 2019
prohibits manufacturers from engaging in this practice.41,42
Preventing this practice is projected to save about $3.1 billion over the next
decade.43,44
A third set of technical
changes to MDRP relates to data and reporting. The rebate calculation relies on
price data and product information submitted by manufacturers to CMS.
Misclassified drugs or inaccurate price information in these files affects the
rebate calculation. A number of policy proposals would strengthen price
enforcement mechanisms at the federal level to improve the accuracy of
information and ensure appropriate rebates are paid and allow for penalties for
reporting inaccurate information. Proposals include providing the Secretary of
HHS with the authority to reclassify drugs that are incorrectly classified,
increasing oversight of rebates by requiring CMS to conduct regular audits of
drug manufacturers’ pricing information, providing the Secretary additional
authority to impose a penalty on manufacturers that submit inaccurate
information and increasing the penalties for not complying with reporting
requirements.45,46
Increasing
Supplemental Rebates
Due to the structure of
the MDRP, state levers to negotiate supplemental rebate agreements have
primarily been limited to PDL placement. In addition, as statutory rebates have
increased over time, state supplemental rebates have grown much more slowly and
declined as a share of total rebates.47,48 In
recent years, states have been exploring new approaches to try to obtain larger
supplemental rebates from manufacturers.
Some policy proposals
focus on increasing purchasing power to negotiate additional supplemental
rebates. For example, aligning PDLs across FFS and MCOs may provide more
leverage for a state negotiating with a manufacturer. As of fiscal year 2019,
at least 17 states had a uniform PDL for one or more drug classes.49
California has proposed negotiating rebates across all state programs, not just
Medicaid.50
PBMs have been another
area of focus for state efforts to increase supplemental rebates. Much activity
in this area involves increased transparency about PBM practices by, for
example, requiring PBMs to report their discounts, rebates and profits to the
state to ensure that the state is receiving the maximum rebates possible. More
than half of states have passed a law addressing some aspect of PBM practices
and transparency.51
Other states have enacted or are considering broader transparency laws to
obtain pricing information from manufacturers in an effort to better understand
prices paid by different parties in the production and payment chain for
prescription drugs.
Other state efforts
include expanding the scope of supplemental rebates—for example, by extending
supplemental rebates to MCOs—or adding an inflationary component to
supplemental rebates.52,53
Value-Based
Purchasing
A final way in which
states have been pursuing supplemental rebates is through value-based
purchasing. With the increasing number of high-price, breakthrough drugs that
cost hundreds of thousands up to millions of dollars, states are examining ways
to pay for these therapies within their constrained budgets. Some states are
pursuing alternative payment methods, or paying for value, as possible
solutions. States have authority to pursue these agreements, but they must fit
within the parameters of the MDRP. Given the best price provision, which leads
manufacturers to hesitate to offer lower prices, states have opted to craft
their arrangements under the umbrella of supplemental rebates, which are exempt
from best price. While referred to colloquially as “value-based payment,” most
agreements so far do not condition payment on clinical outcomes.
As of October 2019, six
states have approval to implement alternative payment models via supplemental
rebates.54
These states include Louisiana and Washington, both of which are implementing a
subscription model (also known as the “Netflix model”) to pay for hepatitis C
drugs. Some legislative proposals would provide further authority for states to
enter into risk-sharing, value-based contracts with manufacturers for
outpatient drugs that are potentially curative treatments.55,56
These agreements would be treated like supplemental rebates for the purpose of
calculating AMP and best price.
Opting
Out of the MDRP
Some policy discussion in
recent years has been about opting out of or eliminating the MDRP, which
essentially creates an open formulary, to allow states to use closed
formularies in Medicaid, under which only specific drugs in each therapeutic
class are covered. Some argue that allowing states to implement these
“widely-used commercial tools”57
would allow states to negotiate greater rebates, because each manufacturer
would want their drug to be included as one of the few drugs for the
therapeutic class. The Trump Administration has expressed interest in this
approach, and the FY 2019 budget called for a new Medicaid demonstration
authority to enable up to five state Medicaid programs to create their own
formularies and negotiate directly with manufacturers instead of participating
in the Medicaid Drug Rebate Program.58,59
States are showing limited interest in the idea, though some states have
expressed interest in a closed formulary that still obtains MDRP rebates.60,61
However, as of October 2019, the federal government has not approved waiver
requests for this approach.62
Changing
Rebates or Prices in Other Programs
While not specifically
targeted to Medicaid or MDRP, policy proposals to change the structure of
rebates or prices in Medicare and the private market also affect Medicaid.
These indirect effects occur because many proposals affect list prices or AMP,
which in turn affect Medicaid rebate calculations. For example, in early 2019,
the Trump administration released a proposed rule that would have excluded
rebate payments by drug manufacturers to PBMs, Medicare Part D plan sponsors,
and Medicaid managed care organization (MCO) plan sponsors from “safe harbor”
protections that make these payments exempt from anti-kickback penalties. The
Administration withdrew the idea, but analyses of the proposal at the time
indicated that it would increase Medicaid spending. This outcome would occur
through decreased list prices by manufacturers, which would lower the
inflationary Medicaid rebate.63
Similarly, proposals (such as those made by the Administration64
and by House Democrats) to align Medicare drug prices more closely with drug
prices in other countries could have implications for Medicaid rebates and
ultimately Medicaid drug spending by changing drug list prices. Policy changes
that would allow the federal government to negotiate Medicare prices also may
have implications for Medicaid, depending on how the price applies to the wider
marketplace and the prices used to set Medicaid rebates.65
Summary
The MDRP helps offset
federal and state costs of most outpatient prescription drugs dispensed to
Medicaid beneficiaries and ensures access to medication for Medicaid
beneficiaries. While gross prescription drug costs continue to grow, the
Medicaid Drug Rebate Program has held net Medicaid costs largely flat over the
past few years. There continues to be growing national attention around the
issue of high drug prices and as a result, both states and the federal
government are considering a variety of policies to address prescription drug
costs. Because of the key role Medicaid plays in providing drugs for
beneficiaries and setting the floor for prices, it is important for policy
makers to understand the implications of any proposed policies for the rebate
program.
This work was supported
in part by Arnold Ventures. We value our funders. KFF maintains full editorial
control over all of its policy analysis, polling, and journalism activities.
No comments:
Post a Comment