Wyatt Koma Follow @KomaWyatt on
Twitter, Juliette Cubanski Follow @jcubanski on
Twitter, Gretchen Jacobson, Anthony Damico, and Tricia Neuman Follow @tricia_neuman on
Twitter Published: Dec 02, 2019
Each year, Medicare beneficiaries in private
Medicare Advantage plans and Part D stand-alone prescription drug plans (PDPs)
have the opportunity to change plans during the annual open enrollment period
(October 15 to December 7). Medicare’s private plans vary significantly from
each other and can change from one year to the next, which can have a significant
impact on enrollees’ coverage and costs. The Centers for Medicaid &
Medicare Services (CMS) encourages beneficiaries to shop for Medicare Advantage
and prescription drug plans to potentially save money on prescriptions or get
new benefits.
Understanding how Medicare private plan
markets are working is increasingly important for both beneficiaries and the
Medicare program overall. Many presidential candidates and policymakers have
proposed establishing a public program, modeled on Medicare, to expand
coverage, while others want to expand the role of private plans within Medicare
itself. To inform these discussions, this analysis examines the share of people
enrolled in Medicare Advantage prescription drug plans (MA-PDs) and PDPs who
switched plans for the following year during the open enrollment periods
between 2007 and 2016, the most current year available for analysis of Medicare
private plan switching rates. This analysis excludes enrollees with low-income
subsidies; more detailed methods are described below.
·
Overall, a small share
of MA-PD and PDP enrollees without low-income subsidies (8% and 10%,
respectively) voluntarily switched to another plan during the 2016 annual open
enrollment period for the 2017 plan year (Figure 1).
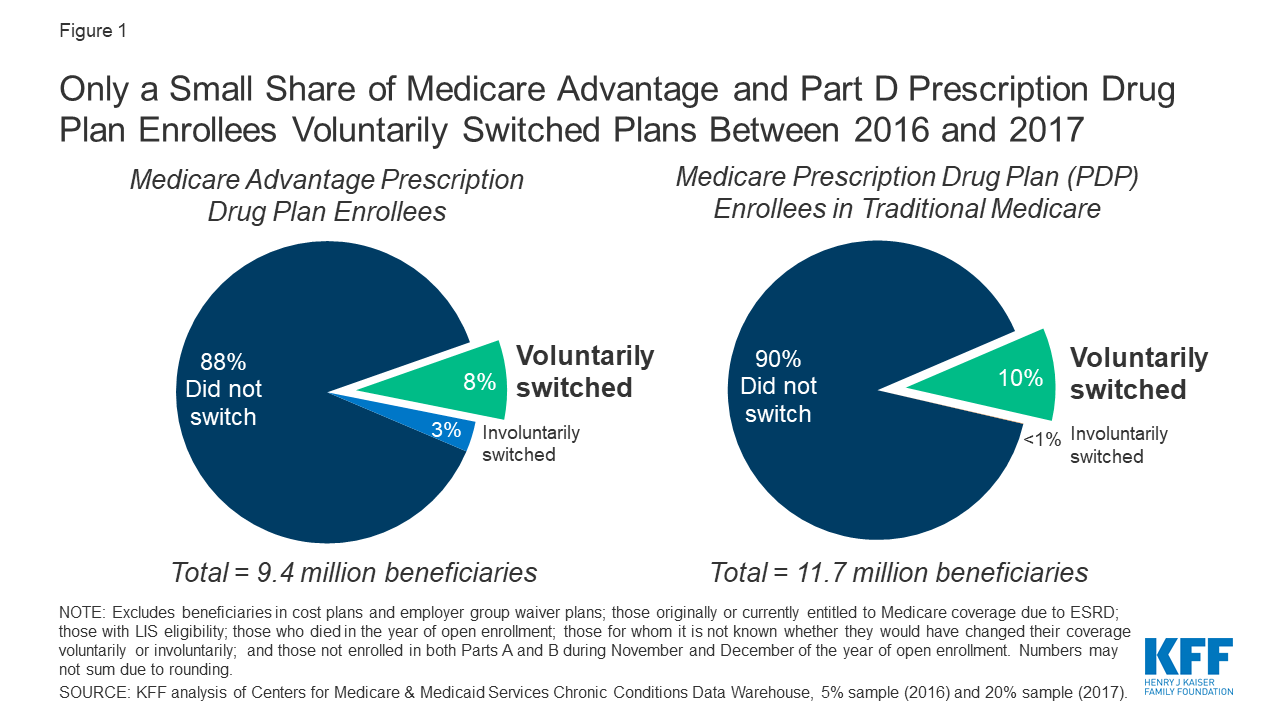
Figure 1: Only a Small
Share of Medicare Advantage and Part D Prescription Drug Plan Enrollees
Voluntarily Switched Plans Between 2016 and 2017
·
Among 9.4 million
MA-PD enrollees without low-income subsidies, 7.6 percent (710,000
beneficiaries) voluntarily switched to another MA-PD during the 2016 open
enrollment period for 2017, and another 0.9 percent (90,000 beneficiaries)
switched from an MA-PD to traditional Medicare (with a PDP). Among 11.7 million
PDP enrollees without low-income subsidies, 8.3 percent (980,000 beneficiaries)
switched to another PDP and another 1.7 percent (200,000 beneficiaries)
switched to an MA-PD during the 2016 open enrollment period for 2017. (A very
small share of Part D enrollees switch to MA-only plans or traditional Medicare
without Part D coverage; they are excluded from this analysis.)
·
A substantial majority
of Medicare private plan enrollees have not voluntarily switched plans in any
given year over the time period of this analysis. During the open enrollment
periods between 2007 and 2016, the share of enrollees without low-income
subsidies voluntarily switching plans for the coming year ranged between 6 and
11 percent for people in Medicare Advantage drug plans, and between 10 and 13
percent among those in stand-alone drug plans (Figure 2).
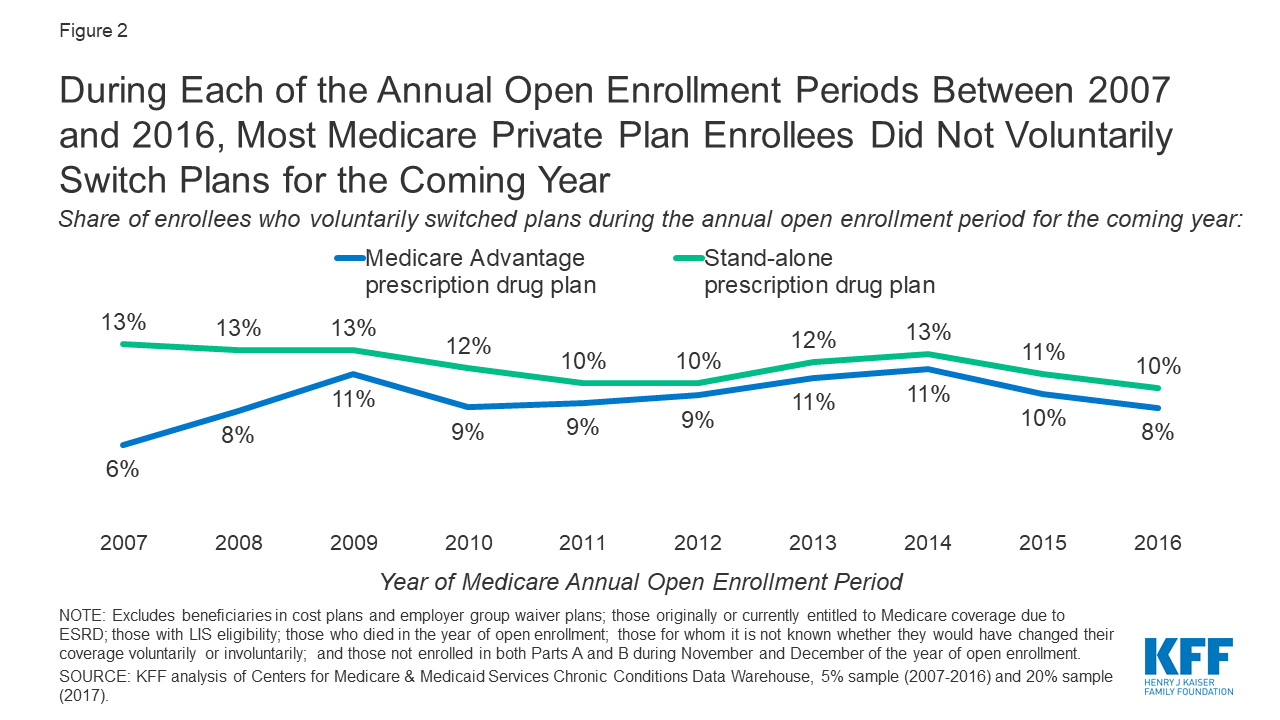
Figure 2: During Each
of the Annual Open Enrollment Periods Between 2007 and 2016, Most Medicare
Private Plan Enrollees Did Not Voluntarily Switch Plans for the Coming Year
·
Some share of people
who did not switch in any given year are beneficiaries who were enrolled in
plans that exited the market and were “crosswalked” (i.e., automatically
enrolled) by their plan sponsor into a new plan the following year. This means
their plan is different from the previous year, but they did not voluntarily
choose a new plan. For the 2017 plan year (corresponding to the 2016 open
enrollment period), this comprised roughly 8 percent of MA-PD enrollees and 3
percent of PDP enrollees. Another small share of enrollees involuntarily
switched MA-PDs (3%) or PDPs (<1%) because their plan exited the market for
2017 and they were not automatically crosswalked into a new plan.
·
Based on our analysis
of the Medicare Current Beneficiary Survey, in 2017, more than one in three
(35%) Medicare beneficiaries living in the community said it is very or
somewhat difficult to compare Medicare options, and this share increased among
beneficiaries in fair or poor self-reported health (44%) and with five or more
chronic conditions (40%).
·
In 2017, nearly half
(45%) of people on Medicare living in the community said they rarely or never review
or compare their Medicare options; the share was substantially higher among
beneficiaries ages 85 and older (57%).
Discussion
With an average of 28 Medicare Advantage plans and 28 stand-alone Part D plans available
to beneficiaries in 2020, beneficiaries have dozens of plan options from which
to choose. Relatively low rates of plan switching during the open enrollment
period could indicate that beneficiaries are generally satisfied with their
current plan and therefore have little motivation to compare and switch plans,
or they may be actively choosing to remain in their plan after comparing other
available options.
But, low switching rates could also indicate
that many beneficiaries find the process of comparing plans
too challenging, are unaware of the open enrollment period, or have
limited confidence in their ability to choose a better plan. Both Medicare
Advantage and stand-alone drug plans can vary significantly in terms of
premiums, deductibles, cost sharing, provider and/or pharmacy networks, and
drugs covered, among other plan features. Comparing all of these factors
simultaneously is the best way to maximize value and lower costs, but it is
also time consuming and challenging, especially for beneficiaries with
cognitive impairments or serious health needs.
Our finding that a majority of MA-PD and PDP
enrollees stay in the same plan during the annual open enrollment period may
not be a concern, but it raises a question as to whether “stickiness” leads to
avoidable costs, or unrealized benefits, for a large share of the Medicare
population. The finding that nearly half of all Medicare beneficiaries say they
never or rarely compare plans suggests that many beneficiaries may be unaware
of important differences across plans that could have a significant impact on
their coverage, costs, and, in the case of Medicare Advantage plans, access to
certain providers. This is not surprising given the sheer number of Medicare
private plans now available and the many ways in which they differ. Given that
some presidential candidates and policymakers are discussing proposals to build
on Medicare and the marketplace model or to broaden the role of private plans
in Medicare, understanding the barriers that people on Medicare experience will
continue to be important for policy discussions.
Wyatt Koma, Juliette Cubanski, Gretchen
Jacobson, and Tricia Neuman are with KFF. Anthony Damico is an independent
consultant.
No comments:
Post a Comment